Importance of Work and the Role of Vocational Rehabilitation
Participation in employment promotes many positive qualities for individuals with disabilities. Employment is regarded as an essential means of independent living and is often how people represent themselves in society. Vocational identity is an important aspect of personal identity that often reflects individual personality, social norms, and family upbringing (Dunn et al., 2008). For individuals with disabilities, employment has also been shown to provide opportunities for increased engagement in meaningful community participation and social activity, thus promoting recovery, independence, and a sense of pride and accomplishment (Dean et al., 2018; Dunn et al., 2008). For this reason, helping consumers find competitive employment has been the primary goal of the vocational rehabilitation (VR) system.
Various VR services have been shown to be effective in assisting consumers with diverse disabilities deal with employment barriers and achieve employment goals (Chiu et al., 2013; Nevala et al., 2019; Wehman et al., 2014). However, the effectiveness of services for consumers who discontinue services without successful case closure is not typically considered. It has been found that roughly 50% of consumers within the VR system left prior to successful employment, and many cases were closed due to consumers’ refusal of services or failure to cooperate (Dutta et al., 2017). This information can provide important implications for current VR services: (a) many consumers entering the VR system might have difficulties in forming good working relationships with the rehabilitation counselors (RCs), and (b) RCs need further preparation to address the consumers’ complex needs that prevent service engagement.
In this vein, integrating knowledge about trauma and trauma-informed care (TIC) into training for RCs, as well as the service process, may help address the issue of early dropout. Forming a strong working relationship with healthcare providers is often a significant challenge for those with a higher level of traumatic experiences. These challenges are exacerbated when practitioners lack the essential knowledge and sensitivity to create safe environments, which is crucial in preventing retraumatization (Substance Abuse and Mental Health Services Administration, 2014a). The inability to accommodate the complex needs of those with traumatic experiences often leads to consumers’ inadvertent retraumatization and causes heightened sensitivity to perceived threats or criticisms in service settings (Huo et al., 2023). This manifests as avoidance or resistance in therapeutic relationships and can ultimately cause consumers to drop out. This issue is particularly relevant in the field of rehabilitation counseling, considering the significantly high prevalence of traumatic experiences among individuals with disabilities. To address this, RCs must possess advanced knowledge in trauma and trauma-informed care. However, this crucial aspect has often been overlooked in the field of rehabilitation counseling.
Trauma and Vocational Rehabilitation Services
Trauma, according to SAMHSA, “results from an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or threatening and that has lasting adverse effects on the individual’s functioning and physical, social, emotional, or spiritual well-being” (2014b, p. 2). Trauma-related symptoms are often the result of psychological reactions to overwhelming adverse events including accidents and serious injury, physical and sexual abuse, unexpected or sudden death of a loved one, experiencing violent crimes, and natural disasters. Under this broad scope, experiencing trauma is not rare in current society. The prevalence data of trauma varies across studies, but roughly six out of ten men and five out of ten women experience at least one traumatic event throughout their lives (Benjet et al., 2016; Felitti et al., 1998; U.S. Department of Veterans Affairs, 2018). In a large-scale mental health survey conducted globally, almost 70% of more than 60,000 adults across 24 nations reported they have experienced at least one potentially traumatic event in their lifetime (Kessler et al., 2017). Further, empirical studies have shown the increased vulnerability of individuals with disabilities to exposure to trauma and trauma-related symptoms (SAMHSA, 2014b).
Prevalence of Trauma in Individuals With Disabilities
The empirical studies focused on the trauma of individuals with disabilities have demonstrated how common traumatic experiences are in disability communities. The prevalence of traumatic experiences seems much higher in individuals with disabilities compared to individuals without disabilities (García-Cuéllar et al., 2023; Hahn et al., 2014; Petersilia, 2001). Specifically, aspects of disability in and of itself can be associated with traumatic events, from experiencing disaster to accidents that potentially result in serious injury or physical impairments such as a traumatic brain injury (TBI), paralysis, or amputation. People with disabilities, often facing serious medical diagnoses and treatments, are at an increased risk of experiencing medical trauma due to their more common and sometimes intensive interactions with healthcare systems (Hall & Hall, 2013). Moreover, individuals with disabilities are at higher risk to be victims of interpersonal trauma including physical and sexual abuse, violence, and bullying. From a review of victimization of individuals with disabilities, it was found that the risk to be victimized by violence, abuse, and/or neglect for individuals with disabilities is 4 to 10 times higher than for individuals without disabilities (Petersilia, 2001). In a study conducted with 34,563 participants, adults with physical disabilities and mental health impairment were associated with 19 to 93% increased risk of victimization by intimate partner violence (IPV; Hahn et al., 2014). In a recent systematic review, the increased risk of victimization of women with disabilities from IPV was consistently reported across 26 empirical studies (García-Cuéllar et al., 2023). Individuals with intellectual disabilities have also been at high risk for experiencing trauma in social contexts (McNally et al., 2021). Recently, with the onset of the pandemic, concerns regarding elevated physical/emotional violence and discrimination toward individuals with disabilities have been raised due to social isolation and lack of resources or support for coping (Lund, 2020; Lund & Ayers, 2022).
Potential Impact of Trauma on the Mental Health of Individuals With Disabilities
According to empirical evidence, pervasive impacts of trauma on individuals’ physical, emotional, and behavioral health can create unique barriers for individuals with disabilities to obtain and maintain employment, as well as remain engaged throughout the VR service process. Regardless of the type of trauma, the impacts of mental health-related symptoms following trauma are not only limited to mental health concerns, but also expand to psychosocial functioning. Trauma survivors with posttraumatic symptoms including depression, anxiety, somatization, dissociation, and affect dysregulation are more likely to experience negative emotions and interpersonal issues in work settings due to recurring uncontrolled symptoms, feelings of powerlessness, poor boundaries, social isolation, and lack of proper support (Ballou et al., 2015; Bath, 2008; Blustein et al., 2008). Further, the lack of coping resources for individuals with disabilities could contribute to increased severity and duration of posttraumatic symptoms. For example, individuals with limited intellectual capacity may have more difficulties recovering from traumatic events because of limited ability to describe their experiences and emotions, and the potential lack of autonomy over their own lives (McNally et al., 2021).
Potential Impact of Trauma on Employment of Individuals With Disabilities
Previous studies conducted in the field of rehabilitation indicate that traumatic experience itself is associated with employability and work potentials of individuals with disabilities, either directly or indirectly (O’Sullivan et al., 2019). Strauser and colleagues (2006) examined the relationship between trauma and career development among college students with disabilities and found that higher levels of trauma symptoms are adversely associated with students’ career development process including work personality, vocational identity, and career thoughts. More recently, studies in rehabilitation counseling have started focusing on the impact of trauma in populations with specific psychosocial impairments. A few studies have focused on the impact of trauma on people with specific types of disabilities such as substance use disorders, intellectual disability, autism, and traumatic brain injury (Burke et al., 2009; Capezza & Najavits, 2012). Findings from this research support the idea that addressing trauma in clients with disabilities can improve employment outcomes and psychosocial functioning for individuals with disabilities.
Potential Impact of Trauma on Service Engagement of Individuals With Disabilities
Decades of extensive research in healthcare services have identified retraumatization as a leading cause for client drop-out across various healthcare settings (Jennings, 2004). Individuals who have experienced trauma are often prone to developing generalized threat schemas, making them highly sensitive to even seemingly irrelevant stimuli that could potentially remind them of past traumatic events. Surprisingly, even stimuli seemingly irrelevant to their trauma can trigger posttraumatic reactions and avoidance behaviors. Clients with a history of trauma may perceive therapeutic relationship as hierarchical and even oppressive, rather than supportive (Harris & Fallot, 2001). They often find these relationships anxiety-provoking or even threatening, while failing to recognize the connection between their past traumas and their current experiences in the service provision setting (Kazelman & Stavropoulos, 2012). In such situations, even minor behavioral cues or word choices from counselors can trigger posttraumatic reactions, causing the client to disengage from the services provided. Therefore, without advanced understanding of trauma and its effects on the client, VR counselors are at risk of inadvertently retraumatizing their clients. This diminishes service engagement, thereby reducing the overall effectiveness of the service.
Need for Trauma-Informed Care in Rehabilitation Counseling
In response to the pervasive impact of traumatic experiences, the primary goal of TIC is to incorporate an understanding of trauma and its impacts into every facet of the service delivery system to create a safe and facilitative environment for clients (Lang et al., 2016; Levenson, 2017; Substance Abuse and Mental Health Services Administration, 2014a). Unlike approaches that focus solely on specific models of trauma treatment, TIC aims to coordinate the continuum of care and establish collaborative processes. This is to better address the multifaceted needs of clients who have experienced trauma, rather than merely offering trauma-specific services (SAMHSA, 2014a). Implementing TIC can be particularly beneficial in the field of VR, especially for serving individuals with disabilities. By employing a trauma-informed approach, VR counselors can prevent retraumatization and enhance the overall engagement of clients in employment services.
Training Need for Trauma-Informed Care in Rehabilitation Counselors
According to guidelines from the Substance Abuse and Mental Health Services Administration, workforce training on trauma and trauma-informed care is a cornerstone for implementing TIC in human care settings (SAMHSA, 2014a). A systematic review by Bryson et al. (2017) supports this, emphasizing that comprehensive training and quality support for staff are critical for enhancing their behavior, knowledge, and beliefs about TIC. Well-trained staff can articulate clients’ experiences in a common language and identify appropriate interventions.
Given the strong interrelationship between trauma and disability, it is crucial for VR counselors to receive proper training in understanding the impact of trauma on individuals with disabilities. This is essential for effective intervention in rehabilitation service settings. Indeed, the principles of TIC align well with the holistic, biopsychosocial, and strength-based approaches commonly used in the field of rehabilitation (O’Sullivan et al., 2019; Ranjbar & Erb, 2019). Through training, providers can identify and mitigate potential triggers, thereby preventing retraumatization while fostering safe environments and supporting client autonomy throughout the service provision process (Reeves, 2015). Studies have shown that TIC-trained practitioners improve patient-centered interactions and satisfaction (Oral et al., 2016). Additionally, trust-based relationships built on TIC principles enable consumers to feel empowered and more comfortable discussing traumatic experiences (Reeves, 2015). In summary, to prepare RCs for the effective integration of TIC into VR practices, a comprehensive training program should be implemented, including a specialized curriculum focused on trauma, its consequential impact, and the core principles of TIC in the context of disability.
The increasing importance of trauma education can be found in the updated Council for Accreditation of Counseling and Related Educational Programs (CACREP) standards. In the 2016 standards, trauma and trauma-informed approaches were highlighted in only two out of eight core curriculum areas (CACREP, 2016). The latest 2024 standards expand this focus, incorporating the effects of trauma and the necessity for trauma-informed approaches across five distinct areas including social and cultural identities and experiences, lifespan development, career development, counseling practice and relationship, and assessment and diagnostic processes (CACREP, 2024). This change in the CACREP standards indicates a more comprehensive understanding of trauma’s effects. It is now acknowledged not only as an influencing factor in mental health, but also as a significant element affecting key psychosocial domains throughout an individual’s developmental trajectory.
While TIC is promising as a foundational framework for effective VR service, it is clearly time to examine RCs’ training experiences, as well as the practical application of trauma-focused approaches in their day-to-day work. To provide basic information on these areas, this study aims to shed light on VR counselors’ training experiences related to trauma. Further, this study explores how post-graduate training experiences are associated with the actual utilization of trauma focus and knowledge in day-to-day practices in VR counseling. Finally, the Technology Acceptance Model (TAM 2; Venkatesh & Davis, 2000) is used as a theoretical framework for examining this association.
Technology Acceptance Model (TAM 2). The Technology Acceptance Model (TAM; Davis, 1989) explains the acceptance and usage of new technology, with an initial focus on voluntary adoption. Addressing the model’s early limitations in explaining involuntary use, Venkatesh and Davis (2000) revised TAM, modified to TAM 2, enhancing its application in both voluntary and mandatory situations (Chuttur, 2009; Lai, 2017). This revised version more thoroughly elucidates how external conditions shape users’ perceptions of usefulness and ease, influencing attitudes and intentions, which ultimately drive actual technology usage.
While the TAM was originally designed to understand the acceptance process of new technology, its applicability has extended to other areas of social research and proven its usefulness in explaining the adoption and usage of new knowledge or services in non-technological, intangible forms. For instance, the TAM 2 has been effectively applied in studies predicting genetic counselors’ adoption of new theories and models, as well as in examining community patients’ acceptance of new services offered by local pharmacies (Heinlen et al., 2019; Persson et al., 2023).
Purpose of Study
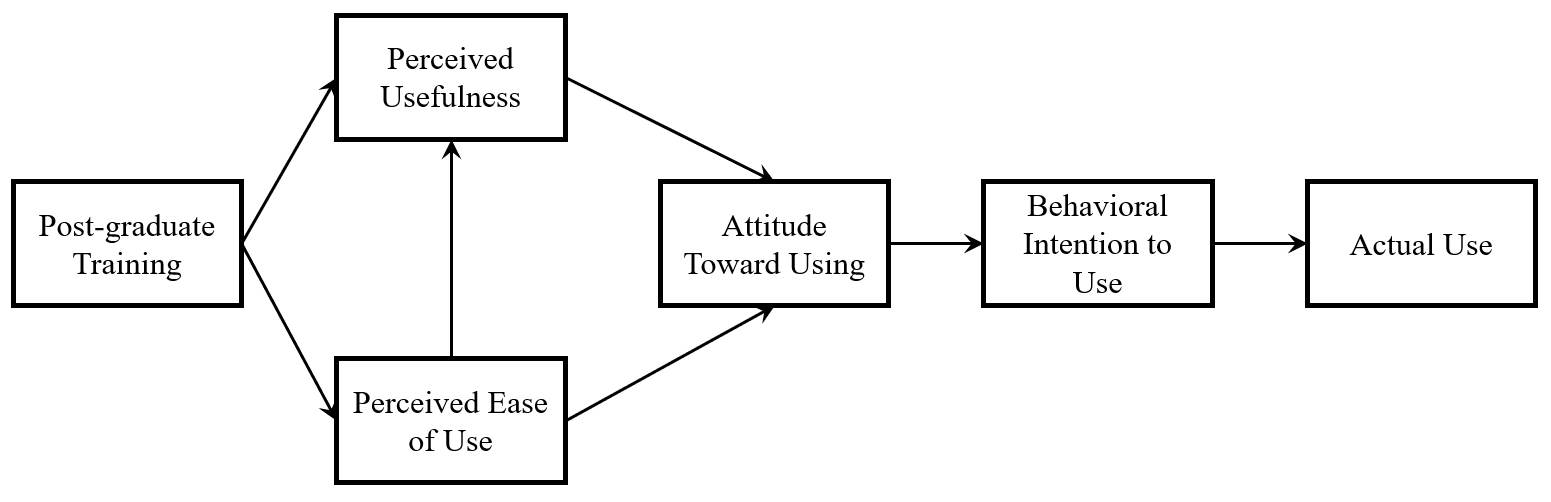
The primary purposes of this study are to (a) examine the training experiences of VR counselors in the area of trauma and TIC and (b) investigate how VR counselors’ training experiences come to connect with actual use of trauma knowledge and trauma-focused approach in practice. According to TAM 2, external variables indirectly influence actual utilization of the new information through a series of direct and indirect relationships among perceived usefulness, perceived ease of use, attitudes toward usage, and behavioral intentions. Based on the theoretical assumptions, the path model was hypothesized and tested to understand the association between post-graduate training and the actual implementation of trauma-focused approaches in VR counseling practice. Therefore, the research has three specific objectives:
-
To identify the number of training hours and the sources of training (e.g., pre-service and in-service training) received by VR counselors in the area of trauma and TIC
-
To test the overall fit of the path model with the collected data
-
To evaluate the strength of relationships among training experience and TAM variables that influence the actual use of trauma/trauma-informed care approaches.
The hypothesized model in this study is structured based on priori specifications, the detailed paths among variables are depicted in Figure 1.

Methods
Participants
Demographics
Data for the present study was gathered via the survey distributed through the Vocational Rehabilitation Technical Assistance Center for Quality Employment (VRTAC-QE) listserv. Out of 170 vocational RCs who completed survey, one entry was excluded for reporting post-graduate training hours that exceeded the threshold of two standard deviations from the mean. Analyses were performed on the responses of 169 participants. The mean age of the participants was 46 years (SD = 10.36; range: 25-68). Most of the participants were White (79.3%). A little less than half of the participants live and work in a suburban area (42.0%). Approximately half of the participants reported working for the general State VR program agency (47.9%). Twenty-four participants work for the combined State VR program agency (14.2%). The demographic characteristics of the participants are summarized in Table 1.
Measures
The trauma and TIC needs assessment survey was designed by the researchers, incorporating items based on TAM 2 (Venkatesh & Davis, 2000). Variables used in the current survey encompassed demographic factors, trauma-related training history, and the RCs’ perspectives on the application of trauma knowledge in their professional practice. The survey was divided into three main sections. The first section gathered information on demographic factors such as gender, age, race, ethnicity, geographic location, professional affiliation, and years of professional experience in the field. The second section of questions solicited information on RCs’ training history in trauma and TIC, exploring aspects like duration, level, and source of training. The third section delved into the RCs’ attitudes and perceptions regarding the incorporation of trauma knowledge and considering consumers’ trauma histories in the provision of VR counseling service.
The five items included in the third section aimed at measuring various constructs related to TAM 2. Initially, these items were developed by a single researcher in accordance with conceptual labels and construct definitions of TAM 2. Then, the two other researchers on the research team reviewed the draft items, and revisions were made based on a collaborative discussion among all three researchers. Finally, an external scholar, who is an expert in the field of VR, was consulted to further refine and finalize the questionnaire. The finalized questions in this section measured perceived ease of use, perceived usefulness, attitude toward paying attention to consumers’ trauma, behavioral intention to utilize trauma knowledge, and actual use of trauma knowledge in counseling. Responses were measured using a 5-point Likert scale, ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). A higher score on this scale indicates a greater level of engagement in the process of intentional or behavioral aspects of integrating and applying trauma-informed practices within daily practices. The overall internal consistency reliability (Cronbach’s alpha) of these five items was .76 for the current study. The survey was distributed for a month in spring 2022 using the VRTAC-QE listserv and VRTAC-QE Facebook page. Information regarding the survey was also distributed via the listserv operated by the National Technical Assistance Center on Transition-Collaborative (NTACT: C).
Data Analysis
Statistical Package for Social Scientists (SPSS) 26.0 was used to identify research participants’ demographic characteristics, means and standard deviations of research variables, internal consistency of measures, and correlation coefficients among them. Path analysis with bootstrapping (n = 5,000; Preacher & Hayes, 2008) was performed to test the hypothesized TAM of trauma-focused approach. All model estimations were conducted with AMOS 18.0 using maximum likelihood estimation. In addition to chi-square goodness-of-fit, the model fit was examined using alternative goodness-of-fit indices: (a) χ2/df, (b) comparative fit index (CFI), (c) Tucker-Lewis Index (TLI), (d) Bentler and Bonett’s normed fit index (NFI), and (e) root mean square error of approximation (RMSEA). Values within the range of 1 to 3 indicate a good fit for χ2/df. CFI, TLI, and NFI bigger than 0.90 indicate good fit, and RMSEA smaller than 0.05 indicate good fit (Kline, 2015). The statistical significance of direct, indirect, and total effects was tested based on 95% bias-corrected confidence intervals around the standardized estimates.
Results
Descriptive Analysis
Means, standard deviations, skewness, kurtosis, and intercorrelations among the research variables are detailed in Table 2. Data normality was confirmed with the values of skewness falling within the range of -2 to 2 and those of kurtosis within -7 to 7 (Bryne, 2010; Hair et al., 2010). In terms of TAM 2 constructs, participants rated high in perceived usefulness of TIC (M = 4.40, SD = .75); moderate in ease of use (M = 3.67, SD = .97); moderately positive in attitude (M = 3.94, SD = 1.03); high in behavioral intention (M = 4.06, SD = .90); moderately high in actual use (M = 3.90; SD = .86). The average number of post-graduate training hours was 9.71 (SD = 11.13). The intercorrelations among variables ranged from 0.04 to 0.61, indicating no concerns regarding multicollinearity.
Trauma-Related Training History
Training history indicated that most participants have had some form of training in trauma or TIC-related topics in the past. Breaking the graduate or undergraduate-level training down, 52.1% reported receiving this training at the bachelor’s level, a mere 1.2% at the master’s level, and 7.1% at the doctoral level. Only 31 participants (12.4%) indicated they have never received any training in these topics, while 46 participants (27.2%) chose not to disclose their level of training. The data also revealed a strong inclination toward post-graduate training, with 137 participants (81.1%) reporting such training in their professional careers. However, the average number of post-graduate training hours is 9.71 (SD = 11.13), in contrast to an average professional experience of 14.88 years (SD = 10.37). Regarding the source of their professional training, most participants cited continuing education units (CEUs) as the primary medium, accounting for 40.8% (n = 69) of responses. Conference or workshop training followed at 24.3% (n = 41), and workplace or agency-offered trainings accounted for 13.6% (n = 23). Table 3 contains data related to training history of participants.
Path Analysis
Path analysis was employed to examine the hypothesized relationships between post-graduate training and the variables within the Technology Acceptance Model (TAM 2), as well as the indirect effects of each predictor variable. The original model showed a significant chi-square statistic, χ2(7, N = 169) = 25.41, p < .001. Alternative fit tests yielded the following: χ2/df = 3.63, CFI = .91, TLI = .80, NFI = .88, and RMSEA = 1.25, indicating that the model fit with the data was less than adequate. Based on these results, the original model was reviewed for modification.
A review of the research model (see Figure 1) based on existing empirical evidence and theoretical frameworks suggests that the model may not adequately capture the complex interrelationships among its constructs. Specifically, while the TAM 2 does not propose a direct relationship between perceived ease of use and behavioral intention to use technology, the Unified Theory of Acceptance and Use of Technology (UTAUT) model (Venkatesh et al., 2003) postulated that ease of use is a strong predictor of behavioral intention. Accordingly, the researchers assumed that ease of use significantly impacts behavioral intention.
Moreover, the Theory of Planned Behavior (TPB; Ajzen, 1988) offers additional insight by suggesting that ease of use can directly influence actual behavior. TPB operationalizes “perceived behavioral control” as an individual’s belief in their ability to control a behavior, which has been interpreted in various studies as the ease or difficulty of implementing a specific behavior (Wallston, 2001). Several studies have shown that perceived behavioral control can influence a variety of health-related behaviors under different conditions (Hamilton et al., 2020; McEachan et al., 2011; Sheeran et al., 2003).
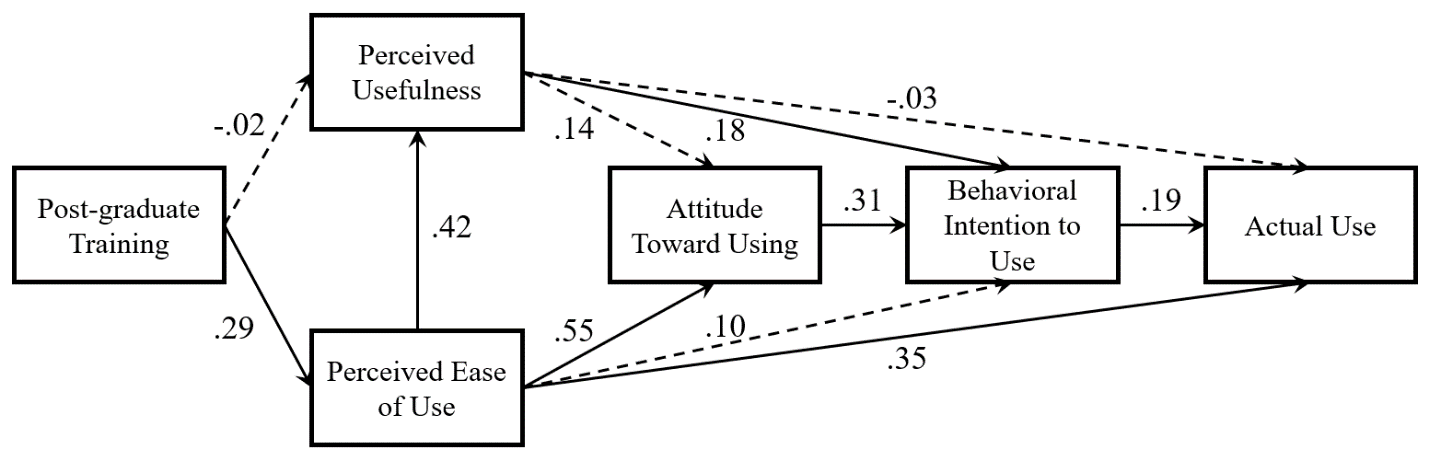
Lastly, from the TAM literature, a direct relationship between perceived usefulness and actual usage is posited. Several studies have found that the perceived usefulness of an intervention or technology is highly correlated with its actual usage. In one research study examining TAM in using protective behavioral strategies for alcohol use behaviors, perceived usefulness of the protective strategies was associated with actual use of the prevention strategies in both the present and the future (Fairlie et al., 2021). Based on these theoretical and conceptual reasoning, three direct paths were added into the respecified model: (a) direct effect of perceived ease of use on the behavioral intention to use; (b) direct effect of perceived ease of use on the actual use; and (c) direct effect of perceived usefulness on the actual use. The graphical representation of the respecified model is illustrated in Figure 2.
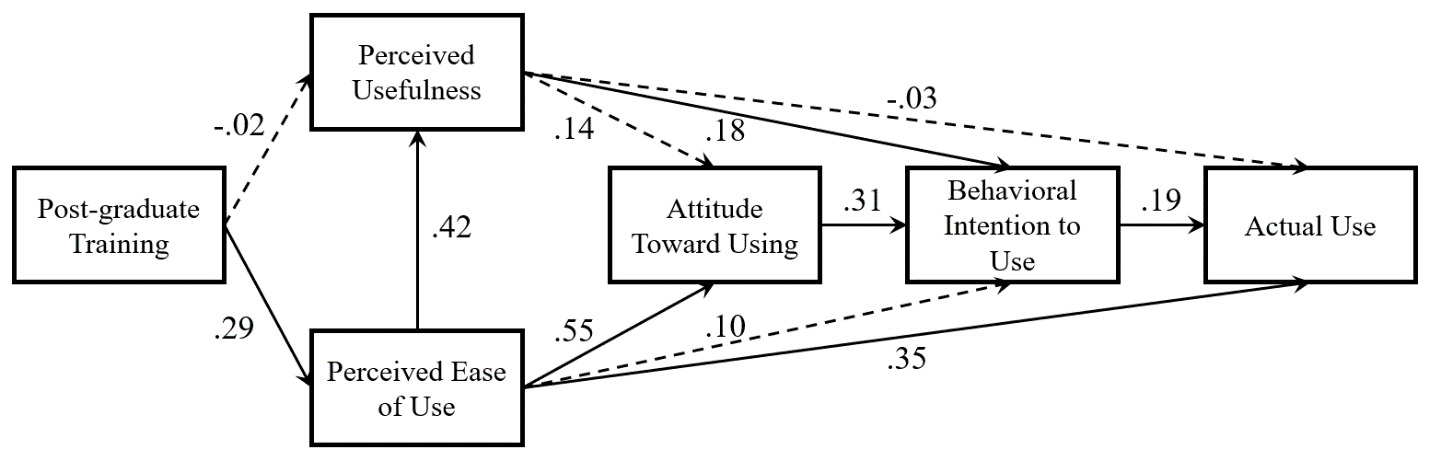
The results from the goodness-of-fit test for the respecified model indicate excellent model fit. Specifically, the chi-square statistic was non-significant at χ2(4, N = 169) = 4.10, p = .392, which generally suggests a good fit between the hypothesized model and the observed data. Further, alternative fit indices also supported the adequacy of the model: χ2/df = 1.03, CFI = .99, TLI = .99, NFI = .98, and RMSEA = .012. These results confirm that the respecified model closely fits the empirical data. Regarding the explanatory power of the model, the squared multiple correlation coefficients (R2) varied between .08 and .38 for different constructs in the model. Specifically, training in trauma and TIC accounted for 8.2% of the variance in perceived ease of use. Variables associated with perceived usefulness explained 17.4% of its variance. Attitude toward using trauma-focused approaches was explained by variables accounting for 38.4% of the variance. For behavioral intention to use, 24.0% of the variance was explained, and for actual use, the predictors accounted for 19.9% of the variance.
In path analysis, variance explained presents how much of the variance in a dependent variable is captured by the independent variables and paths in the model. In social science research, a lower R-square value, like 0.1 (or 10%), is often acceptable if the predictors or explanatory variables are statistically significant (Ozili, 2023). The current results show that the ability of the research model to explain the variance in different constructs ranges from low to moderate, with the highest explanatory power (38.4%) for attitude toward using and the lowest (8.2%) for perceived ease of use.
Detailed information on the relationships among the research variables is presented in Table 4. The research model reveals both direct and indirect effects as follows. Post-graduate training had a significant direct effect on perceived ease of use (β = .286, p < .001), but not on perceived usefulness (β = -.017, p > .05). Perceived ease of use showed a significant direct effect on perceived usefulness (β = .422, p < .001), attitude toward using (β = .548, p < .001), and actual use (β = .351, p < .001). However, it had no significant effect on behavioral intention (β = .103, p > .05). Perceived usefulness exerted a significant direct effect on behavioral intention (β = .185, p < .05), but not on attitude toward using (β = .140, p > .05) or actual use (β = -.031, p > .05). Attitude toward using had a significant direct effect on behavioral intention (β = .313, p < .01). A significant path was observed between behavioral intention and actual use (β = .194, p < .05).
For the indirect effects among variables, post-graduate training had an indirect influence on perceived usefulness (β = .121, p < .001) mediated by perceived ease of use. It also indirectly affected attitude toward using (β = .171, p < .001) via perceived ease of use and perceived usefulness. Additionally, it influenced behavioral intention (β = .102, p < .01) and actual use (β = .117, p < .01) through the interplay of all Technology Acceptance Model (TAM 2) variables. Perceived ease of use was indirectly related to behavioral intention (β = .268, p < .01) through its relationship with attitude toward using. However, non-significant indirect paths were observed between ease of use and both attitude toward using (β = .059, p > .05) and actual use (β = .058, p > .05). The indirect effects of perceived usefulness on behavioral intention (β = -.044, p > .05) and actual use (β = .044, p > .05) were not statistically significant. Attitude toward using had a significant indirect effect on actual use (β = .061, p < .05), mediated by behavioral intention.
Discussion
The present study examined the training experiences of RCs in areas pertinent to trauma and TIC. Research findings show that 60.4% (n = 102) of the survey participants had education/training in their graduate or undergraduate training, while only 8.3% (n = 14) reported that this education/training was provided by their graduate programs. Concerning post-graduate (in-service) training, 81% (n = 137) participated in trauma-relevant training. However, the total hours of training were limited (M = 9.71, SD = 11.13) over an average career span of nearly 15 years (M = 14.88, SD = 10.37).
The study also explored TAM tailored to RCs’ training in trauma and TIC. Although the initial research model did not align well with the data, the respecified model exhibited excellent goodness-of-fit, thereby confirming its utility as a framework to understand how post-graduate training influences RCs’ actual application of their trauma-relevant knowledge in practice. Approximately 20% of the variance in RCs’ actual use of trauma knowledge was explained by the respecified model. Consistent with prior literature, post-graduate training was found to be a significant determinant in the actual utilization of trauma-relevant knowledge. It influenced both direct and indirect relationships with all TAM variables, including perceived ease of use, perceived usefulness, attitude toward using, and behavioral intention. Specifically, while post-graduate training directly impacted perceived ease of use, it had an indirect effect on perceived usefulness through its relationship with perceived ease of use. This pattern suggests that training may directly enhance RCs’ belief that trauma knowledge is easy to incorporate into their practice, which, in turn, increases their expectations regarding the usefulness of these approaches for improving service quality. Essentially, training could support RCs’ self-efficacy or confidence, thereby elevating expectations surrounding the utility of trauma-focused knowledge.
In this context, the important role of perceived ease of use as a mediator between training and other TAM variables became evident. It fully mediated the relationship between training and perceived usefulness. Additionally, its direct effects were identified on attitude toward using, and actual use behaviors. Though the direct link between perceived ease of use and behavioral intention was not statistically significant, an indirect effect was significant when mediated by attitude toward using and perceived ease of use. Overall, these findings suggest that trained RCs are more likely to be more confident in employing trauma-relevant knowledge, which is likely to enhance their perception of its effectiveness, openness to its application, intentionality in its use, and actual implementation of trauma-focused approach in daily practice.
Implications for Rehabilitation Counseling
The intersectionality of disability and trauma represents a critical but under-explored area within the field of rehabilitation counseling. Given the elevated risk of trauma exposure among individuals with disabilities, as well as the disabling impact of trauma, it is critical for both RCs and researchers to integrate these intertwined topics to promote service quality. In this regard, this study holds significant implications for professionals, educators, and researchers serving this vulnerable population, especially in the area of VR counseling.
The study revealed that 159 VR counselors nationwide reported receiving fewer than 10 hours of training on trauma and TIC over an average professional span of 15 years. This deficiency in training is alarming, particularly considering existing research in healthcare fields that connects traumatic experiences with lower rates of service engagement and higher drop-out rates (Jennings, 2004). Consumers who have encountered traumatic events may perceive power imbalances in professional relationships as threatening, leading to their withdrawal from the service. Furthermore, many of those may not make the connection between their past traumas and their current experiences within service environments (Kazelman & Stavropoulos, 2012). To foster a safe and accommodating environment and facilitate service engagement for those consumers, RCs must have comprehensive knowledge about trauma to adjust service environment, set appropriate boundaries, and offer continuous psychoeducation throughout the service delivery process. Achieving this level of competency necessitates specialized training focused on the trauma, particularly in the context of VR service.
The study has important implications for efforts to increase capacity among the field to serve individuals with disabilities who are trauma survivors. Federal agencies support numerous centers whose primary purpose is to provide technical assistance toward increasing the capacity of service providers in evidence-based practice. For example, the Vocational Rehabilitation Technical Assistance Center for Quality Employment (VRTAC-QE) is supported by the Rehabilitation Services Administration to, “is to increase the knowledge and skills of state VR agencies and community partners that help people with disabilities achieve quality employment and career advancement, with emphasis on competitive integrated employment” (VRTAC-QE, 2023). In providing technical assistance, centers such as the VRTAC-QE may need to evaluate pre-existing training in TIC, or even more broadly, in any area of capacity building, and commit to providing remedial-to-advanced training in those areas a priori to promote successful integration and implementation of skills. For example, customized employment services were codified under the Workforce Innovation and Opportunities Act. Several recent studies have indicated limited success, in part due to limited use of customized employment services by state VR agencies (Kim, Inge, et al., 2023; Kim, Riesen, et al., 2023). The VRTAC-QE and other centers providing technical assistance in this area may need to consider lack of training as a barrier to the implementation of this service. Likewise, in terms of TIC, similar barriers to implementation exist (e.g., lack of training, lack of knowledge) and this study provides a clear pathway regarding methodology to increase capacity and ultimately implementation of this and other services.
According to SAMHSA’s guidelines for implementing TIC, training is foundational for developing a trauma-informed workforce (SAMHSA, 2014a). Based on these guidelines, there are pivotal areas of trauma-related knowledge that are essential for VR counselors and RCs to successfully implement TIC in their practices. First, VR counselors need a well-rounded understanding of the various dimensions of trauma. This includes recognizing the different types of trauma individuals may experience, their prevalence, and their multifaceted impact on overall health and functioning. Such a comprehensive understanding builds the groundwork for counselors to better assess and meet the unique needs of consumers with disabilities. Second, RCs should be trained in conducting trauma assessments. These evaluations should be designed to identify the specific needs and challenges of consumers with disabilities and cover a broad range of psychosocial issues. Such assessments should consider the psychosocial impacts of trauma on key life domains such as education and employment. Lastly, VR counselors must be familiar with available trauma-specific treatments and interventions. This knowledge enables them to make informed referrals for specialized trauma treatment if needed, ensuring that consumers get the appropriate care they require. This is particularly important for consumers who have complex needs stemming from both disability and trauma.
This study also provides valuable insights into the development of training programs aimed at helping VR counselors incorporate trauma knowledge into their practices. The results indicate that training positively influences RCs’ perceived ease of use of trauma-related knowledge. Importantly, this perceived ease of use indirectly impacts the perceived usefulness of such knowledge. As such, building counselors’ confidence in applying trauma-related knowledge and skills should be central to effective training initiatives that aim to encourage actual use. In this context, employing pedagogical strategies like experiential learning, case studies, and peer activities can be particularly beneficial. For instance, experiential components, such as role-playing or group activities, can facilitate the application of theoretical knowledge in a simulated environment. Likewise, case studies can offer realistic scenarios that challenge VR counselors to improve their problem-solving and critical thinking skills. Peer activities can offer a platform for collaborative learning, enabling the exchange of unique insights and approaches that have been cultivated in different practice environments.
Finally, there is a need for scholarly efforts to explore the complex interplay between disability and trauma. Existing empirical evidence suggests that trauma is often associated with factors like poverty, marginalization, and oppressed identities that frequently overlap with disability too (SAMHSA, 2014a). However, these intersections remain largely unaddressed in disability research. Greater focus on this area can inform RCs’ understanding of the prevalence and potential consequences of trauma, including retraumatization sources in work settings and preventative strategies. Such research can help VR counselors have the knowledge needed to tailor their services more effectively, therefore fulfilling the complex needs of individuals with disabilities who have also experienced trauma.
Limitations and Future Research Directions
There are several limitations that should be noted in this study. First, the sampling method and related bias should be considered. The participants were recruited through online platforms. This could limit the generalizability of the sample to the people who have accessibility and ability to use the Internet to complete the survey. Also, due to the relatively small sample size, the research outcomes may not generalize to the RCs working in diverse settings. In addition, the survey was developed by the researchers for the current study, and each construct included in the analysis was measured using a single item. Issues of reliability, validity, and comparability of the measure should be considered in interpreting and generalizing the results. Further research is needed to examine the psychometric properties of the instrument. One of the limitations also lies in the absence of detailed information on participants’ educational backgrounds and details of pre-service training, critical aspects considering our focus on trauma training across different academic and professional levels. Addressing these elements in future research is essential for a more accurate understanding of the current trauma training in the field of rehabilitation counseling, especially in the current context of varied educational requirements for VR counselors post-WIOA. Future research can include more variables to improve the nuanced understanding of the adoption process of new approach. For instance, subjective norms can be a variable under the Theory of Planned Behavior to better understand the implementation of TIC. Investigating how these norms in workplace settings influence professionals’ willingness to use TIC, especially considering its perceived usefulness, would be insightful. Finally, the current study focuses on rehabilitation counselors working in vocational settings and distributed the survey through the VRTAC-QE listserv. However, the sample predominantly consists of RCs from state vocational systems. This potential overrepresentation may not fully reflect the diversity of perspectives and experiences in a broader field. Future research should aim to include diverse work settings to further the generalizability of research outcome.
Conclusion
The profession of rehabilitation counseling is anchored by the commitment to serve individuals with disabilities as effectively as possible. In pursuit of this mission, it is crucial and timely to incorporate trauma-related training into the realms of practice, education, and research. This will improve the overall support for individuals with disabilities and facilitate quality service delivery. RCs have a specialized role in facilitating positive outcomes for those with disabilities, who are often at heightened risk for encountering traumatic events. By enhancing their understanding and expertise in trauma-related issues through professional training, RCs will be better equipped to foster meaningful engagement with clients in VR services.
Author Note
The contents of this paper were developed under a grant (H264K200003) from the Vocational Rehabilitation Technical Assistance Center for Quality Employment, U.S. Department of Education. However, those contents do not necessarily represent the policy of the U.S. Department of Education or U.S. Department of Health and Human Services, and you should not assume endorsement by the Federal government.