Disclosure of disability represents a pivotal decision process that significantly impacts societal inclusion for people with disabilities. It involves navigating complex interpersonal and institutional dynamics that can either facilitate or hinder access, support, and belonging. Valle et al. (2004) characterized disclosure as an ongoing decision-making process involving considerations of why, who, what, and when to disclose, as individuals continuously weigh potential benefits and risks that vary across different social contexts. This process is multifaceted, influenced by a combination of personal and environmental factors.
The consequences of disclosure vary depending on the context. In educational settings, disclosure is often instrumental in securing accommodations and support services, with students expected to disclose their disabilities to receive the assistance necessary for academic participation (Cole & Cawthon, 2015; Eccles et al., 2018). However, such disclosures may also expose students to risks of isolation or stigma. In employment contexts, disclosing a disability during job applications has been shown to reduce the likelihood of receiving positive responses from employers (V. Pearson et al., 2003), and similar challenges have been documented when disclosing to graduate programs (Salzer, 2022). In personal relationships—such as friendships or romantic partnerships—disclosure involves additional considerations around identity, trust, and vulnerability. These examples illustrate how disclosure decisions are shaped not only by individual circumstances but also by broader contextual dynamics.
Research examining disability disclosure has identified several key personal factors, including confidence in managing disclosure conversations, severity of one’s disability, and the need for accommodations and equal access (Gignac et al., 2021; Hammel et al., 2015; Von Schrader et al., 2014). Environmental factors include the attitudes of potential disclosure recipients, organizational culture, and disability-related policies and legislation. The interaction between these personal and environmental factors (e.g., an individual’s fear of stigma in conjunction with an employer’s lack of disability awareness) can heighten the perceived risks of disclosure (Black et al., 2015; Martin, 2010).
Visibility, Stigma, and Severity
A central consideration in disclosure decisions is the visibility of the condition. Individuals with non-apparent conditions (e.g., mental illness, HIV/AIDS) may hesitate to disclose due to concerns about invoking devaluing attitudes and discrimination. However, keeping their condition a secret can lead to unwanted psychological effects, such as identity ambiguity and constant vigilance related to potential discovery (Pachankis, 2007). In contrast, those with more apparent conditions (e.g., mobility impairment requiring the use of a wheelchair) may find it difficult to conceal their condition (Allen & Carlson, 2003) and feel compelled to discuss their disability to prevent others from making erroneous assumptions.
Stigma represents another critical factor in disclosure decisions. Stigma encompasses stereotypes (oversimplified misconceptions), prejudice (negative evaluations), and discrimination (differential treatment) (Corrigan & Watson, 2002). Disclosure decision-making research suggests that the desire to avoid stigma plays a central role in decisions about whether to disclose a stigmatized identity (Chaudoir & Fisher, 2010). This motivation is often linked to efforts to preserve self-esteem and mitigating negative perceptions across social, educational, and professional contexts (Allen & Carlson, 2003). In the context of higher education and disability services, concerns about stigma and anticipated negative social reactions have been identified as barriers influencing students’ decisions to disclose disabilities and seek accommodations (Marshak et al., 2010; May & Stone, 2010).
Severity pertains to the extent to which a disability affects an individual’s functioning and quality of life (Brady et al., 2016; Lindsay et al., 2018; Mitra et al., 2017). Severity can range from mild, where symptoms may be manageable without accommodations, to very severe, where substantial support is necessary for daily functioning. These gradations influence not only a person’s lived experiences but also how others perceive them, often shaping responses from peers, educators, or employers. Individuals with more severe disabilities may face higher social and structural barriers, including limited autonomy in disclosure decisions or heightened fear of negative consequences. Research has shown that increasing severity often correlates with greater perceived stigma and reduced access to equitable opportunities (Pelleboer-Gunnink et al., 2021; Werner & Shulman, 2013). These dynamics highlight the importance of attending to disability severity when examining disclosure experiences and the social context in which such decisions are made.
Dimensions of Disclosure: Motivations, Emotional State, and Anticipated Outcomes
The self-disclosure literature identifies several important dimensions that shape disclosure behaviors. Disclosure motivations, as described in the Functional Theory of Disclosure originally articulated by Derlega and Grzelak (1979), suggest that individuals disclose personal information for various reasons, including social control, relationship building, and self-clarification. This foundational framework has been extended and applied in contemporary research on interpersonal and mediated disclosure processes (Bazarova & Choi, 2014). Garcia and Crocker’s (2008) work with individuals experiencing depression provides a framework specifically relevant to stigma disclosure, distinguishing between ecosystem motivations (focused on contributing to or supporting others) and egosystem motivations (concerned with protecting one’s self-image). Their research demonstrated that individuals with egosystem goals disclosed less and experienced lower psychological well-being when they did disclose. Conversely, those with ecosystem goals disclosed more frequently and experienced greater psychological well-being during disclosure. This suggests that the underlying motivations for disclosure significantly impact both disclosure decisions and the psychological consequences.
Recent research by Cipollina et al. (2022) has further refined our understanding of disclosure behaviors by examining disclosure directness—the degree to which one explicitly discusses their stigma during a disclosure experience. Their findings suggest that more direct disclosures (involving explicit and outright discussion of the stigma) elicit more engaged, supportive, and satisfying responses from disclosure recipients. Many individuals, however, use less direct disclosure methods, such as suggesting or hinting at their stigma to “test the waters” and ascertain recipients’ attitudes (Jones et al., 2016; Orne, 2011). This research suggests that disclosure style, not just the decision to disclose, significantly influences disclosure outcomes.
The emotional state involved in disclosure represents a second important dimension. Drawing on Bandura’s self-efficacy theory (1997), confidence and anxiety significantly influence disclosure behaviors. Individuals who feel confident in their ability to navigate disclosure situations are more likely to share personal information, whereas those experiencing anxiety may be more hesitant (Capa-Aydin et al., 2018). These emotional states are shaped by past successes or failures in disclosure experiences and by perceptions of the social environment. Successfully managing disclosure situations tends to reduce anxiety and build confidence (Hier & Mahony, 2018), while negative experiences can increase anxiety and discourage future disclosures (Fong & Krause, 2014).
The final dimension involves anticipated outcomes of disability disclosure, characterized by feelings of empowerment, relief, or regret. For some, disclosure leads to a sense of empowerment through openness about their disability, boosting self-esteem and affirming personal identity (Spreitzer, 1995). Additionally, disclosure may bring relief as the emotional burden of secrecy is lifted (Greene, 2009). However, others may anticipate negative consequences such as stigma, discrimination, or damaged relationships, resulting in regret following disclosure (Chaudoir & Fisher, 2010).
Building on self-disclosure literature, the present study investigates how disability-related factors—namely stigma, visibility, and severity—intersect with key dimensions of disclosure behavior. Specifically, we examine how the severity of a condition predicts perceived visibility and anticipated stigma, and whether visibility is associated with anticipated stigma. We also explore how these factors influence disclosure motivations, emotional state, and anticipated outcomes. To guide this investigation, the study addresses the following research questions:
-
How does disability severity relate to perceived visibility and anticipated stigma?
-
What is the relationship between perceived visibility and anticipated stigma?
-
How do disclosure motivations, emotional state, and anticipated outcomes differ based on severity, visibility, and anticipated stigma?
-
How do severity, visibility, and anticipated stigma interact to shape disability disclosure behaviors?
Method
Participants
A total of 221 individuals with chronic illnesses or disabilities participated in the study. Participants were required to meet specific inclusion criteria, including being at least 18 years old, residing in the U.S., and self-identifying as having a disability or chronic health condition. The mean age of the participants was 43.22 years (SD = 13.31). The majority of participants were White/Caucasian (73.8%), followed by African American/Black (10.9%), Latino/a/x or Hispanic (5.9%), two or more (5.4%), Asian (3.6%) and other (0.5%). In terms of gender distribution, 94 participants (42.5%) identified as cisgender men, 104 (47.1%) as cisgender women, 5 (2.3%) as transgender men, 2 (0.9%) as transgender women, and 9 (4.1%) as non-binary/gender non-confirm, while 7 (3.2%) reported other identities. Regarding disability visibility, 42 participants (19%) reported apparent disabilities, while 179 participants (81%) reported non-apparent disabilities. Disability severity varied, with 17 participants (7.7%) reporting mild disabilities, 107 (48.4%) reporting moderate disabilities, 76 (34.4%) reporting severe disabilities, and 21 (9.5%) reporting very severe disabilities. The most frequently reported primary disabilities and health conditions among participants were mental health conditions (28.5%), followed by chronic pain (19%), endocrine disorders (13.1%), neurological issues (9.5%), and mobility limitations (7.7%). The participants identified a total of 16 distinct primary disability and health condition categories, with complete details available in Table 1.
Measures
Single-item measures were employed to assess the concepts of visibility, stigma, severity, and disclosure dimensions. This approach is supported by research demonstrating that single-item measures can be valid and efficient alternatives to multi-item scales for certain research purposes (Diamantopoulos et al., 2012). Although such measures may exhibit somewhat lower reliability compared to multi-item scales, they often demonstrate sufficient predictive validity while reducing participant burden (Fisher et al., 2016). In health and disability research specifically, single-item measures have proven valuable for assessing constructs such as perceived health status and symptom severity (DeSalvo et al., 2006). For this exploratory study, single-item measures were selected to efficiently capture key aspects of each construct while minimizing response fatigue among participants with chronic conditions and disabilities.
Visibility
Participants were queried about whether they would describe their disability or health condition as apparent or non-apparent based on their own experience. This measure utilized a single item where participants indicated whether their condition is apparent or non-apparent. Apparent was defined as the condition being clearly visible or noticeable to others, whereas non-apparent indicated the condition is not readily visible or noticeable to others.
Stigma
Participants were asked to indicate whether they feel their health condition or disability is negatively stereotyped or viewed unfavorably by society. This measure was assessed using a single item where participants selected either Yes or No. Each of these measures was carefully chosen to capture key aspects relevant to the study’s aims and was implemented as a single-item measure for efficiency in data collection and analysis.
Severity
Participants were asked to rate the severity of their disability or health condition based on how significantly it affects their daily life. This measure was assessed using a single item on a 5-point Likert scale, ranging from very mild to very severe. Higher scores indicate greater levels of severity.
Disability Disclosure
Three dimensions of disclosure were examined: disclosure motivations, emotional state, and anticipated outcomes. In the disclosure motivations, we included paired items to assess whether individuals feel obligated to disclose (i.e., “I feel a sense of obligation to disclose my disability in certain situations”) or view it as an autonomous decision (i.e., “The decision to disclose my disability is entirely up to me”). Additional items within the disclosure motivations dimension addressed personal and social aspects of disclosure. From a personal perspective, the item explored how disclosure supports embracing one’s self-identity (i.e., “I disclose my disability to affirm my self-identity”). From a social perspective, the item examined how disclosure enhances relationships with others (i.e., “I disclose my disability to foster better connections with others”). Within the emotional state dimension, items measured affective reactions to perform challenging activities such as disclosure, ranging from feeling confident (i.e., “I often feel confident about disclosing my disability”) to anxious (i.e., “I often feel anxious about disclosing my disability”). The anticipated outcome dimension included items to evaluate feelings of empowerment (e.g., “I often feel empowered after disclosing my disability”), relief (e.g., “I feel relieved after disclosing my disability”), or regret (e.g., “I always feel regretful after disclosing my disability”) following a disclosure experience. Each item is rated on a 5-point scale, ranging from 1 (strongly disagree) to 5 (strongly agree), with participants indicating their level of agreement with statements related to these three areas. Higher ratings indicate strong endorsement of the statements.
Procedure
Once the study protocols were approved by the Institutional Review Board at a university in the Midwest, the sample was collected via Prolific (www.prolific.com), a widely-used crowdsourcing platform for research purposes. We implemented a pre-screening step on Prolific that allowed us to distribute study information exclusively to individuals residing in the U.S. who reported having a disability or a chronic health condition. We then involved potential participants confirming their alignment with the study’s inclusion criteria. After completing eligibility, participants were directed to a consent form detailing the study’s objectives, voluntary participation, confidentiality measures, potential benefits and risks, and incentives. Upon obtaining consent, participants accessed a one-time online survey administered via Qualtrics (www.qualtrics.com). The survey was designed to be completed in 30 minutes, with a median completion time of around 24 minutes. Completion of the survey entitled participants to a $6 incentive payment via Prolific.
To ensure data quality and participant attentiveness, two validation methods were embedded throughout the survey. Some questions directed participants to select specific responses (e.g., “Please choose ‘Agree-2’ for this statement”), while others required consistency in responses to repeated inquiries, such as age verification. Initially, 260 individuals began the survey. Eight participants who completed less than 20% of the survey were removed (completion rate = 96.9%). Additionally, 31 participants who failed the attention validation checks were excluded, resulting in a final sample of 221 participants.
Data Analysis
Data were first screened for missing values and distribution. Skewness and kurtosis levels fell within the acceptable range for a normal distribution. The perceived visibility of one’s condition and the anticipation of stigma were treated as categorical variables. A chi-squared test was used to assess their associations. Logistic regression analyses were conducted to assess if the severity of the condition influenced participants’ perceptions of visibility and their feelings of being stigmatized. Regarding the three aspects of disclosure, differences within each aspect were first assessed for the sample using paired sample t-tests. Subsequently, 2x2 ANOVAs were employed to investigate how participants’ disclosure behaviors, encompassing three dimensions, varied across different groups categorized by visibility (visible vs. non-visible), severity (severe vs. non-severe), and stigma anticipation (anticipated vs. not anticipated). For this analysis, we used median split to dichotomize severity into two categorical levels: high and low.
Results
A chi-squared test showed no significant association between perceived visibility of one’s condition and anticipated stigma, χ²(1) = .12, p = .73, contrary to our initial hypothesis. The logistic regression indicated that severity significantly predicted visibility, χ²(1) = 9.41, p < .01, accounting for 6.7% of the variance (Nagelkerke R²). The Hosmer and Lemeshow test confirmed the adequate fit of the model, χ²(2, N = 221) = .74, p = .69, n.s. Higher severity enhanced the likelihood of the condition being noticeable (odds ratio = 1.99). Similarly, logistic regression further revealed that the severity of the condition significantly predicted anticipated stigma, χ²(1) = 12.25, p < .01, explaining 7.6% of the variance (Nagelkerke R²). The Hosmer and Lemeshow test supported model fit, χ²(2, N = 221) = 1.91, p = .38, n.s. Higher severity levels were linked to an increased chance of expecting stigma (odds ratio = 2.0).
Before exploring the effects of visibility, anticipated stigma, and disability severity on disclosure behaviors, we first assessed whether differences emerged within the dimensions of those three disclosure dimensions (see Table 2). The first dimension, disclosure motivations, included two motivational regulations (the sense of obligation vs. autonomy) and two orientations (self-acceptance vs. the desire to connect with others). Overall, findings indicated that participants were more inclined towards autonomous disclosure of their disability [t(220) = -4.40, p < .01, Cohen’s d=.30], coupled with a stronger motivation driven by social reasons [t(220) = -2.04, p = .04, Cohen’s d=.14]. No significant difference was observed within the emotional state dimension. Regarding the anticipated outcomes, significant differences were found in both the empowered-relieved [t(220) = -6.39, p < .01, Cohen’s d=.43] and the relieved-regretted [t(220) = 5.14, p < .01, Cohen’s d=.35] comparisons. This showed that disclosing one’s condition was more closely associated with feelings of relief than empowerment or regret.
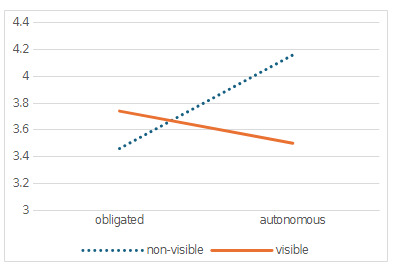
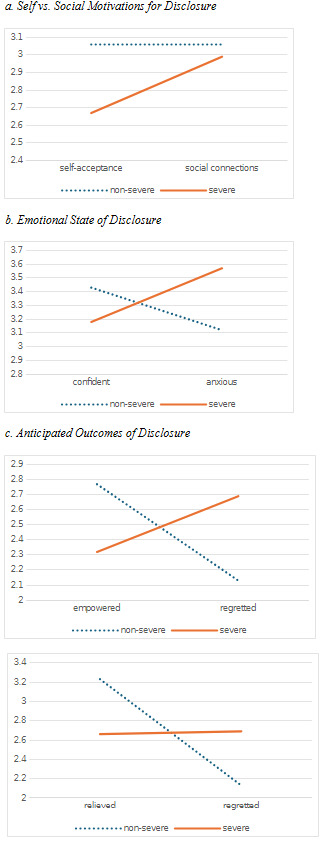
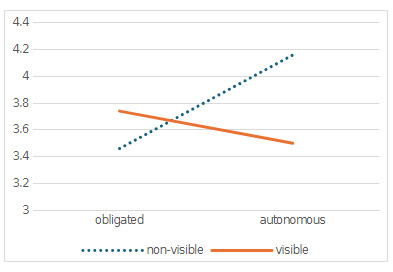
We conducted 2 x 2 repeated measures ANOVA for each disclosure dimensions. Results revealed a significant interaction between disclosure motivations (obligated vs. autonomous) and perceived visibility, [F(1, 219) = 10.12, p < .01, η² = .04] (see Figure 1). Individuals with non-apparent conditions felt less obligated and more autonomously inclined to disclose compared to those with more noticeable conditions. Visibility did not significantly influence the other aspects of disclosure. The severity of the condition interacted with all three disclosure dimensions (see Figure 2, a-c). Specifically, participants with more severe conditions were more driven by social reasons than self-acceptance in their decisions to disclose, in contrast to those with less severe conditions [F(1, 219) = 4.41, p = .02, η² = .02]. Similarly, in terms of the emotional state, individuals with more severe conditions experienced higher levels of anxiety and lower levels of confidence compared to their counterparts with less severe conditions [F(1, 219) = 5.72, p = .02, η² = .03].
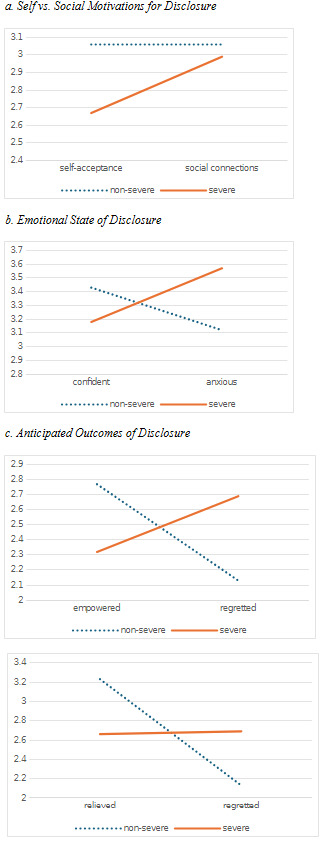
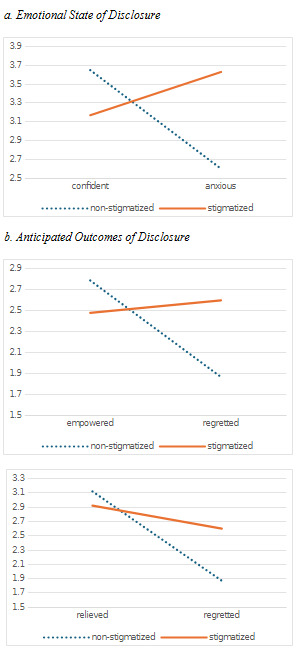
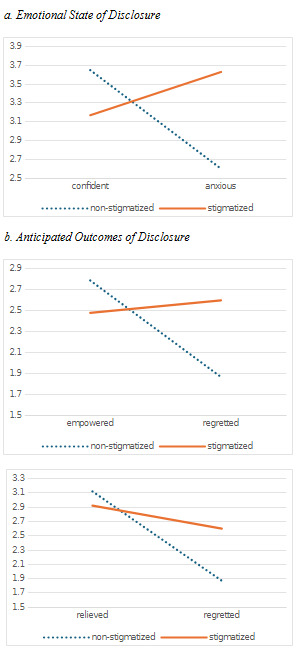
Regarding the anticipated outcomes, individuals with less severe conditions were significantly more likely to report feeling empowered rather than regretful compared to those with more severe conditions [F(1, 219) = 20.42, p < .01, η² = .09]. They also tended to feel more relieved than regretful, contrasting with those with severe conditions [F(1, 219) = 25.35, p < .01, η² = .11. ANOVA analyses also showed significant interactions between the feeling of being stigmatized, emotional state, and anticipated outcomes aspects of disclosure (see Figure 3, a-b). Specifically, for the emotional state, individuals anticipating stigma reported higher levels of anxiety compared to confidence, in contrast to those not anticipating stigma, who exhibited greater confidence than anxiety [F(1, 219) = 25.08, p < .01, η² = .10]. In terms of anticipated outcomes, participants anticipating stigma were more inclined towards regret over feeling empowered, in contrast to those without such concerns [F(1, 219) = 14.01, p < .01, η² = .06]. Both groups tended to feel more relieved than regretful post disclosure. The endorsement towards regret was more pronounced among those expecting stigma [F(1, 219) = 18.74, p < .01, η² = .08].
Discussion
In this study, we investigated the complex interplay between disability severity, perceived visibility, anticipation of stigma, and disclosure behaviors among individuals with disabilities. We were first interested in whether people with severe disabilities were more likely to perceive their disabilities as apparent, and whether they anticipate experiencing stigma due to their disability compared to people with less severe disabilities. Our findings indicated that disability severity is a significant predictor of both perceived visibility and the anticipation of stigma, aligning with prior research suggesting that severe disabilities may be more apparent and subject to greater stigmatization and social biases (Pelleboer-Gunnink et al., 2021; Werner & Shulman, 2013). Next, we were interested in how the perceived visibility of one’s disability related to stigma anticipation, and we found that perceived visibility was not found to be associated with the anticipation of stigma. Other studies highlight how people with apparent disabilities often face negative stereotyping, social avoidance, and discrimination based on their visible appearance (Abes & Wallace, 2018; Barbareschi et al., 2021; Livneh et al., 2014). Similarly, people with non-apparent or hidden disabilities, namely people with psychiatric, learning, and chronic disabilities, also experience stigma in the form of stereotyping, disbelief, and minimization of the impact of disability on one’s life (Flink, 2017; Hendry et al., 2022; Kowalski & Peipert, 2019; Norstedt, 2019). Our findings align with this research, which suggests that people with disabilities experience and anticipate stigma whether they perceive their disability to be apparent or non-apparent. Furthermore, this study expanded our understanding of disclosure behaviors, highlighting nuances within disclosure motivations, emotional state, and anticipated outcomes, and how factors of perceived visibility, severity, and stigma anticipation influence those dimensions of disclosure behaviors.
Disclosure Motivations
Our findings suggest that the decision to disclose one’s disability was more likely to be an autonomous decision, rather than out of obligation. This finding can be contextualized by the American with Disabilities Act (Americans with Disabilities Act of 1990, 1990), which states that people with disabilities are not required to disclose their disability; however, people with disabilities may choose to disclose to receive accommodations in educational or employment settings. This tendency was further nuanced by the finding which highlighted that motivations were primarily driven by the desire to connect with others rather than self-acceptance, indicating a significant social motivation in disclosure decisions. This finding aligns with existing qualitative research which highlight that it is advantageous for people with disabilities to disclose for themselves to connect with others, form solidarity, or even to create space to focus on other topics by “getting disclosure out of the way” (Miller et al., 2019, p. 311).
Visibility also played a critical role in these motivational dynamics. Individuals with non-apparent conditions felt less socially pressured to disclose and more driven by personal choice, suggesting that visibility can alter the perceived necessity and autonomy of disclosure. This contrasts with those with more noticeable disabilities, who might feel a compulsion to disclose due to external expectations, social norms, or forced intimacy (Mingus, 2017; Østerud, 2022). Findings also suggest that individuals with more severe disabilities are more likely to be motivated by social reasons like seeking support or understanding, as opposed to self-acceptance. This finding expands on our previously discussed finding which states that people with severe disabilities are more likely to have an apparent or visible disability. Because others are likely to view more severe disabilities as valid, possibly due to the medical model of disability and the perceived legitimacy of the disability (Godard et al., 2022; Grue, 2023), people with more severe disabilities may not need to rely on others for validation or acceptance of their disability and may instead choose to disclose details about their disability to connect with others.
While other research highlights public stigma as a key driver of disclosure decisions (Blockmans, 2015; Eccles et al., 2018; Kerschbaum et al., 2017), this study finds that the anticipation of stigma did not differentiate the motivational bases for disclosure. This could suggest that individuals anticipating stigma may choose to disclose their disability out of a sense of obligation, such as needing access to accommodations, or from a place of autonomy, such as advocating for people with disabilities or educating others. This lack of differentiation implies that stigma anticipation alone does not sway the underlying motivation but rather the contextual needs or personal values of the individual may play a more significant role. Moreover, the finding that stigma anticipation does not predict whether someone discloses for reasons of self-acceptance versus the desire to connect with others might indicate that these motivations are influenced by intrinsic factors beyond the anticipation of external stigma. Self-acceptance could be driven by internalized positive self-regard and personal growth, whereas the desire to connect with others may be rooted in social needs and the pursuit of interpersonal relationships. These motivations may operate independently of stigma anticipation, highlighting the complexity of disclosure behaviors among individuals with disabilities.
Emotional State
Emotional state, encompassing feelings of anxiety and confidence in relation to disability disclosure, were similar across all participants. Overall, participants reported similar levels of anxiety and confidence across visibility groups, indicating that the perceived visibility of a disability might not be as crucial in affecting the emotional responses associated with disclosure. There is scant research exploring the association between disability visibility and the emotional experience with disability disclosure, however, Chaudoir and Quinn (2010) reported that people with concealable stigmatized identities often experienced positive disclosure experiences when they had ecosystem motivations or motivations to connect with others.
Participants with more severe conditions reported higher levels of anxiety and lower levels of confidence in disclosing their disability. This could be attributed to the increased vulnerabilities and potential negative outcomes associated with disclosing more severe conditions, such as discrimination or social isolation (Freeman et al., 2020). The severity of the disability likely amplifies concerns about being misunderstood, stigmatized, or facing prejudice, leading to heighted anxiety and diminished confidence. This is consistent with research which highlights that the more severe and impactful the disability, the greater the perceived risk and potential repercussions of disclosure, possibly making the process more emotionally taxing for individuals (Baldridge & Swift, 2013). Anticipated stigma also notably impacted mastery of experience, as indicated by feelings of anxiety and diminished confidence. Those expecting stigma demonstrated higher anxiety and lower confidence compared to those who did not anticipate stigma. This aligns with the fear of rejection theory, which posits that the anticipation of negative social reactions can exacerbate stress and reduce one’s sense of belonging in interpersonal interactions (Gerber & Wheeler, 2009). Stigma anticipation likely creates an interpersonal barrier, increasing the emotional burden of disclosure and undermining confidence. Individuals who anticipate stigma might also internalize negative societal attitudes, further eroding their self-assurance and increasing their anxiety (H. Pearson & Boskovich, 2019).
Anticipated Outcomes
The anticipated outcomes of disclosing a disability were significantly associated with feelings of relief, overshadowing feelings of empowerment or regret. This highlights the cathartic effect of disclosure, possibly as a release from the burden of hiding one’s condition or a sense of relief when finding others with similar identities (Pachankis, 2007). The impact of visibility on these feelings was minimal, suggesting the visibility of one’s disability does not significantly alter the emotional outcomes of disclosure. Existing research suggests this effect may stem from the act of disclosure itself, regardless of the visibility of the condition, as disclosure can provide a crucial psychological release that allows individuals to feel more authentic and fully themselves (Miller et al., 2019). This is also consistent with research by Chaudoir and Quinn (2010), who found that revealing concealable stigmatized identities often leads to positive emotional outcomes, primarily relief, due to the reduction of cognitive dissonance and the emotional burden of secrecy.
In contrast, severity and anticipated stigma played more pronounced roles. Disclosure from those with less severe conditions led to feelings of empowerment and relief, potentially because such disclosures involve fewer risks of negative repercussions. Individuals with less severe conditions may perceive the act of disclosure as an opportunity to advocate or educate others as empowering due to the reduced perceived threat of discrimination or adverse reactions, making the process less daunting and more positively reinforcing. Conversely, individuals with severe conditions were more likely to experience regret post-disclosure, reflecting the complex calculus individuals must perform regarding the risks and benefits of disclosing in environments perceived as unsupportive or potentially hostile (Baldridge & Swift, 2013; H. Pearson & Boskovich, 2019).
Furthermore, all participants, regardless of whether they anticipated stigma, tended to feel more relieved than regretful after disclosure. This could suggest that even in the face of anticipated stigma, the act of disclosure provides significant psychological benefits. Relief experienced might stem from the reduction of cognitive dissonance and the emotional burden of secrecy (Chaudoir & Quinn, 2010; H. Pearson & Boskovich, 2019), even if confronted with stigma after disclosure. The relief may also be related to the support and understanding gained from others post-disclosure, which can validate the individual’s experience and reduce feelings of isolation (Gignac & Cao, 2009; Young et al., 2022).
Implications
Our findings reveal several insights that extend beyond existing literature and challenge some current assumptions about disability disclosure dynamics. First, our finding that disability severity predicts both perceived visibility and stigma anticipation, while visibility and stigma anticipation remain unrelated, suggests a more complex relationship than previously understood. This finding calls for a fundamental reconsideration of how disclosure support frameworks are structured. Rather than developing separate approaches for visible versus non-visible disabilities, practitioners should prioritize assessment of perceived severity as the primary factor influencing disclosure experiences. Training or support programs should emphasize that severity perception serves as the key determinant of anticipated stigma and disclosure anxiety.
Second, we found that individuals with non-apparent conditions experience greater disclosure autonomy. In contrast, those with more severe disabilities tend to disclose primarily for social connection rather than self-acceptance, challenging current disclosure counseling practices. Any services or support for disclosure preparation should be redesigned to account for these differing motivational patterns. For individuals with apparent disabilities, the focus might shift from externally driven disclosure to viewing it as an opportunity for meaningful connection rather than merely managing others’ perceptions. For individuals with severe disabilities specifically, coaching should place less emphasis on self-acceptance narratives and instead prioritize leveraging disclosure as a pathway to building supportive relationships.
Third, the unexpected finding that stigma anticipation did not differentiate motivational bases for disclosure contradicts the common assumption that anticipated stigma primarily influences whether disclosure occurs from obligation or autonomous choice. This suggests that broad anti-stigma campaigns may have limited effectiveness in changing fundamental disclosure motivations. Instead, interventions should focus on providing individuals with concrete communication strategies that help them achieve their specific disclosure goals (e.g., connection, accommodation, education) regardless of anticipated stigma. This represents a significant shift from current approaches that often aim to reduce anticipated stigma as a prerequisite for autonomous disclosure.
Fourth, our finding that relief consistently emerges as the dominant emotional outcome of disclosure—even when stigma is anticipated and regardless of disability visibility—provides an important foundation for pre-disclosure counseling. Disclosure preparation should explicitly incorporate this finding, helping individuals anticipate and prepare for this relief response even when they expect negative outcomes. This empirically informed focus on evidence-based emotional preparation represents a novel addition to disclosure readiness training that could significantly reduce pre-disclosure anxiety.
Fifth, our findings regarding emotional states during disclosure, particularly that severity and stigma anticipation, not visibility, predict anxiety and confidence levels, suggest the need for targeted emotional regulation strategies for specific subgroups. Individuals with more severe disabilities would benefit from specialized anxiety management techniques that acknowledge their unique disclosure vulnerabilities, while confidence-building interventions should focus particularly on those anticipating stigma regardless of their disability’s visibility.
These implications move beyond general recommendations for inclusivity and empowerment to provide specific, data-driven directions for reconceptualizing disclosure support based on our study’s unique findings. By implementing these targeted approaches, practitioners can address the actual, rather than assumed, factors that shape disclosure experiences for individuals with disabilities.
Lastly, these findings also carry important implications for rehabilitation counselor educators and training programs. Counselor preparation should incorporate training on how severity and stigma intersect with emotional and motivational aspects of disclosure. Rehabilitation counselor educators can embed these insights into supervision, classroom instruction, and practicum debriefing by encouraging students to develop nuanced, client-centered approaches to disclosure support. Furthermore, the distinction between disclosure motivations (connection vs. self-acceptance) and emotional outcomes (anxiety vs. relief) should inform curriculum content related to disability identity, stigma reduction, and communication strategies. Training future rehabilitation counselors to recognize that visibility alone is not a reliable predictor of stigma or distress will help them develop more individualized and effective counseling interventions.
Limitations and Directions for Future Research
While this study provides valuable insights, several limitations should be acknowledged. First, the reliance on self-reported data introduces the potential for response biases, such as social desirability or recall bias, which may affect the accuracy of the findings. Additionally, the cross-sectional design limits our ability to draw causal inferences about the relationships between disability severity, visibility, stigma, and disclosure behaviors. To address this limitation, future research could benefit from longitudinal studies that track changes in these factors over time, providing a clearer understanding of how these relationships evolve and potentially interact.
A second limitation lies in the generalizability of the findings. Participants were recruited through Prolific, which introduced certain restrictions to sampling. Although the sample was diverse, it may not fully represent the broader population of individuals with disabilities, especially those with less common or more stigmatized conditions. The study’s focus on a specific set of disabilities may also restrict the applicability of the findings to the full spectrum of disability experiences. To enhance the generalizability of future research, it is essential to include a wider range of disabilities and recruit participants through multiple venues, ensuring that the experiences of those with both visible and non-visible conditions are adequately represented.
The study also did not extensively explore the intersectional factors that may influence disclosure behaviors, such as race, gender, and socioeconomic status. Research demonstrates that these identities can compound stigma and significantly shape how individuals experience and navigate disability disclosure. For instance, people of color with disabilities often face racialized ableism that intensifies marginalization (Frederick & Shifrer, 2019), and gender norms can influence how disclosure is perceived or received in various settings (Goodley et al., 2019; Naples et al., 2019). Integrating an intersectional lens into future studies would deepen our understanding of how overlapping identities influence disclosure-related stress, autonomy, and well-being. This would support the development of more inclusive, culturally responsive interventions tailored to the needs of multiply marginalized individuals with disabilities.
Additionally, the use of single item measures raised concerns regarding the validity and reliability of the instruments. It is important to acknowledge that while single-item measures were employed to reduce participant burden, we recognize that complex constructs such as stigma encompass multiple dimensions as outlined in our introduction (i.e., stereotypes, prejudice, discrimination). Our single-item measure of stigma primarily captured participants’ perceptions of how their disability is viewed by society, which may not fully represent all aspects of stigmatization. Although this approach might be appropriate during the exploratory stage of research, future studies should include established multi-item measures for each examined concept to cross-validate the findings and more thoroughly assess each dimension of these complex constructs.
Lastly, given the nuanced findings related to disclosure motivations and the impact of perceived visibility, severity, and anticipated stigma on disclosure behaviors, future studies could delve deeper into these areas. Exploring how different social contexts, or the role of support networks, affect these dynamics would further enrich our understanding and contribute to the development of more targeted and effective support strategies.
Conclusion
This study sheds light on the complex interactions between disability severity, perceived visibility, anticipation of stigma, and disclosure behaviors among individuals with disabilities. The findings highlight the importance of considering both intrinsic and extrinsic factors when supporting individuals in their disclosure decisions. By acknowledging the distinct challenges faced by individuals with more severe disabilities, and by addressing the broader societal attitudes that contribute to stigma, we can create more inclusive environments that empower individuals with disabilities to disclose their identities in ways that align with their personal values and needs. Moving forward, tailored interventions and increased societal awareness will be crucial in promoting positive disclosure experiences and enhancing the well-being of individuals with disabilities.