Introduction
In the United States, persons with disabilities represent more than 60 million adults, approximately 25% of the population with primary disability types reported as hearing, vision, cognition, mobility, self-care, and independent living (Center for Disease Control and Prevention [CDC], 2024). Compared to counterparts without disabilities, those with disabilities experience disproportionate levels of poverty and lack of resources (e.g., social determinants of health [SDOH]) and are at a greater risk of experiencing health disparities directly related to the unequal distribution of social, political, economic, and environmental resources (World Health Organization [WHO], 2021). The SDOH key domains include economic stability, education access and quality, healthcare access and quality, neighborhood and built environment, and the social and community context (e.g., racism, discrimination, violence). The SDOH are largely dependent upon the quality of services a person receives within these domains. Because of existing financial, physical, and structural barriers, persons with disabilities (PWD) are disproportionately impacted by the quality of the SDOH involving social, economic, and political systems. (Friedman, 2021; U.S. Department of Health and Human Services, 2021). Research suggests that persons with disabilities may encounter barriers to accessing education, healthcare services, and employment that can lead to social and economic exclusion and poverty (CDC, 2024). Disability and poverty intersect in ways that mutually reinforce each other, creating cyclical disparity (Krahn et al., 2015). To address the health disparities of PWD, recent actions have been taken at the national level. In June 2021, Executive Order 14035, Diversity, Equity, Inclusion, and Accessibility (DEI&A) in the Federal Workforce, assists PWD to have equitable, accessible and inclusive workplaces (Exec. Order No. 14035, 2021). In February 2022, the National Council on Disability introduced the Framework to End Health Disparities of People with Disabilities, which included designating PWD as a health disparities population under the Minority Health and Health Disparities Research and Education Act of 2000 (National Council on Disability, 2023). In September 2023, the National Institute on Minority Health and Health Disparities (NIMHD) designated PWD as an inclusive population for health disparities research by the U.S. National Institutes of Health. A health disparity designation for PWD provides an opportunity for NIMHD research to address the unmet needs of this heterogeneous population (National Institutes of Health, 2023).
Despite the efforts made in previous years to address the health disparities and inclusive community engagement for PWD, changes in the sociopolitical climate put these efforts at risk. On January 21, 2025, Executive Order 14173, titled “Ending Illegal Discrimination and Restoring Merit-Based Opportunity,” was signed, which aims to revoke efforts made for equal opportunity employment and affirmative action (Exec. Order No. 14173, 2025). Subsequently, on January 29, 2025, Executive Order 14151 titled “Ending Radical and Wasteful Government DEI Programs and Preferencing” was signed, resulting in the termination of DEI and DEIA activities in the Federal government and limiting funding for federal grants supporting inclusive efforts (Exec. Order No. 14151, 2025). Most recently, on July 24, 2025, Executive Order 14321 titled “Ending Crime and Disorder on America’s Streets” was signed, which aims to criminalize persons experiencing homelessness and revert to involuntary institutionalization, thus forcing treatment for persons with mental illness and substance use disorders (Exec. Order No. 14321, 2025). These shifts in policy are likely to impact the civil rights and community inclusion of PWD—marginalizing their voices in shaping policies and interventions.
Additionally, the underrepresentation of PWD in research remains a significant issue impacting health disparity. McDonald et al. (2022) examined 300 clinical trials published in high-impact medical journals and reported that only 2% of the articles reviewed explicitly included persons with intellectual disabilities (ID). Additional studies noted that over 90% of reviewed studies automatically excluded persons with disabilities due to rigid eligibility criteria. The analysis revealed that with minor procedural modifications or accommodations, most of these studies could have safely included participants with intellectual disabilities without compromising research integrity (Feldman et al., 2013). Similarly, Rios et al. (2016) reported that the exclusion of PWD from health research not only limits generalizability but also impairs the ability to develop interventions relevant to a significant portion of the population, particularly given the high incidence of chronic conditions among those with disabilities. DeCormier Plosky et al. (2022) explored the inclusion of PWD in research by reviewing 97 clinical trial protocols across four therapeutic areas. They reported that 85% of the trials permitted broad discretion for investigators to exclude participants, often without clear scientific or ethical justification. Additionally, only 18% of the protocols explicitly allowed the use of assistive technologies or other supports to facilitate participation. Findings reported that when researchers provided justifications for excluding PWD in research, these often focused on concerns regarding consent capacity or ability to comply with study procedures (DeCormier Plosky et al., 2022). This underscores the necessity of employing research methodologies addressing health disparities that emphasize inclusivity and proactively mitigate barriers to participation, including issues related to consent capacity and adherence to study protocols.
Community-based participatory research (CBPR) is a flexible and inclusive framework for addressing disability as a health disparity and advancing social justice and equity through directly involving communities impacted by systemic barriers. CBPR empowers communities, including disability communities, by involving them throughout the research process. As a person-centered approach, CBPR fosters cultural humility and emphasizes co-learning, shared power, and mutual respect. By shifting the power dynamics of traditional research approaches from academic researcher ownership to a community partnership, community members become active participants in co-creating knowledge and driving change. CBPR is pivotal in promoting inclusion, visibility, and accessibility for marginalized communities (Hergenrather et al., 2010; Lee et al., 2018). The six CBPR core components include forming partnerships, assessing community strengths and dynamics, identifying priority concerns and research questions, designing and conducting intervention and or/policy research, feeding back and interpreting research findings, disseminating and translating research findings (Israel et al., 2012; Kendall et al., 2017).
At the core of the CBPR framework is the formation of partnerships with academic researchers and community members. The development of community partnerships frequently originates when academic researchers initiate engagement or further develop existing collaborations with communities or, conversely, when community members or collaborators approach academic researchers to address specific concerns. The partnerships embrace co-learning, shared decision-making, and respect for each partner’s expertise. By including community members in the decision-making process, CBPR aims to balance power among partners and ensure that research is relevant to community needs (Vaughan et al., 2020). Hergenrather et al. (2010) emphasized that researchers must build and foster trust in a community to ensure the representation and engagement of community members’ voices. CBPR mitigates partnership power imbalances to develop culturally responsive research that is accessible, impactful, and creates sustainable change.
Assessing community strengths and dynamics to understand and leverage resources and capabilities within disability communities is a second CBPR core component. The community assessment serves as co-learning between researchers and community members, increasing collective knowledge, building community self-efficacy, and investment in the CBPR process. Governance (e.g., advisory board, steering committee) that includes community representation and leaders have also been utilized for assessment. Through community assessment, the partnership identifies community assets, conducts needs assessments, analyzes community dynamics, and leverages community expertise. The assessment enables CBPR researchers to build upon community strengths, increase community engagement skills and relationship building, and further develop local and institutional knowledge (Collins et al., 2018).
Another CBPR core component is identifying priority concerns and research questions. Unlike traditional research, where researchers or academics from outside the community may often identify the community priority and research questions, CBPR ensures that the community’s expressed lived experiences, needs, priorities, and aspirations drive the research through the partnership. Critical factors in identifying community priorities include the capacity to engage in cultural humility (Collins et al., 2018) and to effectively collaborate with community members, ensuring that researchers’ agendas do not dominate or overshadow the priorities identified by the community (Hergenrather et al., 2010). To identify community priorities and develop research questions, CBPR partnerships have reported creating participant needs assessments, surveys, structured interviews, focus groups, and consensus-building activities (Newman et al., 2014; Nicolaidis et al., 2015; Raymaker et al., 2017).
Among the CBPR core components, designing and conducting research aims to understand the causes of issues develop and test solutions, and influence systems and decision-making processes (e.g., policy research; Israel et al., 2012). By enabling a practice of co-construction, community members are invited to explore and identify research designs of their interest to address community priorities. Researchers can then provide community members with training or mentorship on research designs (Hergenrather et al., 2010). Community members engage as co-researchers, intervention developers, and facilitators. This reciprocal knowledge exchange enhances the research design as the intervention and policy research becomes community-relevant, culturally appropriate, and aligned with community priorities.
The feeding back and interpreting research findings CBPR core component represents the collaborative process of sharing research findings with the community members and engaging them in analyzing and interpreting them to ensure the results are meaningful, accessible, and actionable for the community while respecting their contributions and prioritizing their perspectives. Community members play a crucial role in analyzing and making sense of the research results, ensuring that data is interpreted within the community’s cultural, social, and contextual frameworks (Hergenrather et al., 2010). By engaging community members as equal partners in feedback and interpretation, researchers ensure that findings are relevant, accessible, actionable, and reflective of community priorities.
Disseminating and translating research findings is the final CBPR core component critical in disability-focused research. This process involves collaborative efforts between researchers and community members as partners to ensure findings are presented in agreed-upon venues and that the language is understandable, accessible, relevant, and addresses action (e.g., individual level, community level, agency level, policy). Researchers and community members serve as co-presenters and co-authors (Hergenrather et al., 2010; McDavitt et al., 2016). Translation of research findings into practical applications (e.g., interventions, program and policy changes) contributes to community well-being and the sustainability of community engagement in the research processes.
Purpose Statement
The purpose of this systematic review was to explore the involvement of persons with disabilities (PWD) in the community-based participatory research (CBPR) process. This study aims to analyze how disability communities engaged in the CBPR components of forming partnerships, assessing community strengths and dynamics, identifying priority concerns and research questions, designing and conducting intervention and or/policy research, feeding back and interpreting research findings, and disseminating and translating research findings. We sought to address this with the following research question: How are persons with disabilities involved in the core components CBPR within disability communities? The review sought to explore the contributions of CBPR in promoting social equity PWD throughout the research process.
Method
Review Process
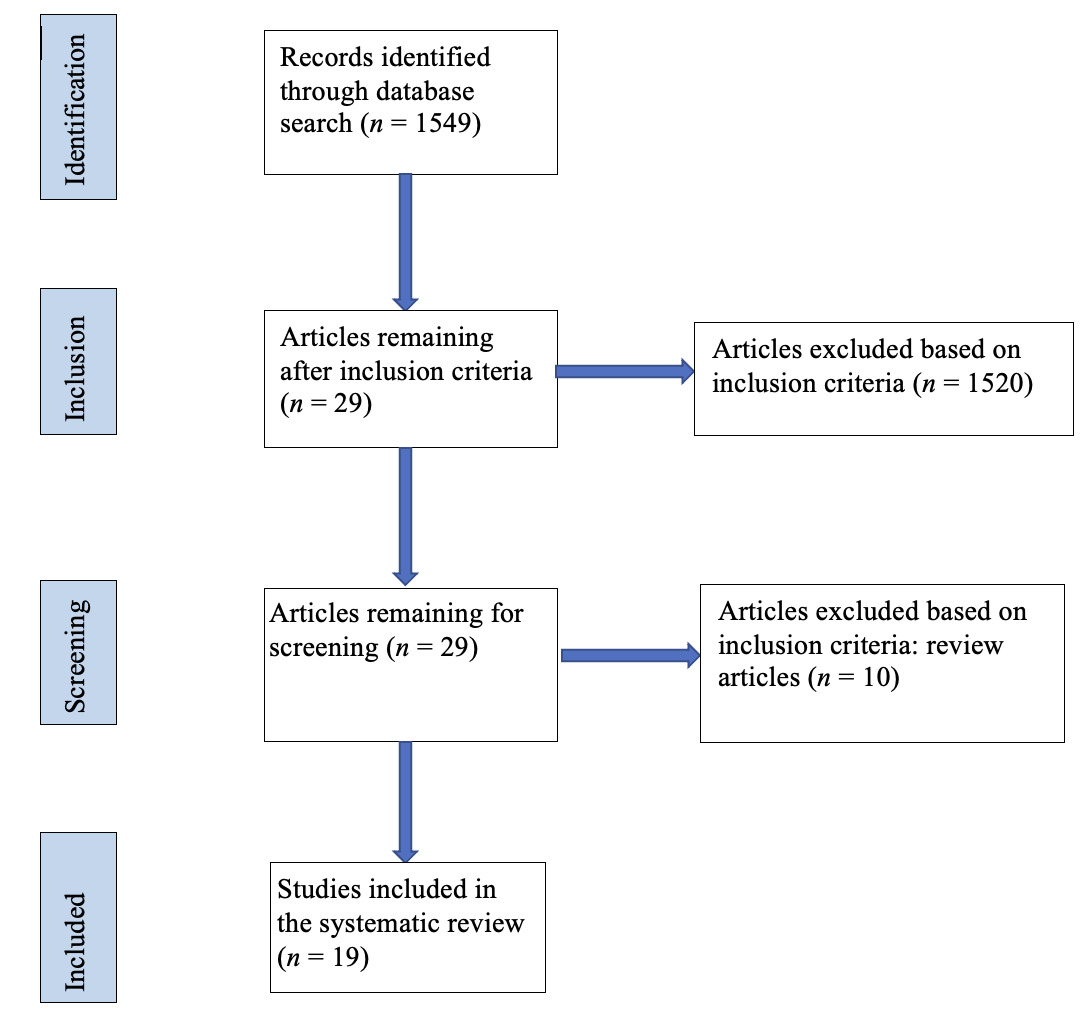
This systematic review was conducted by the authors and included a search of online databases to retrieve articles published from January 1, 2014 through July 31, 2024. Authors facilitated a database search using EBSCO, MEDLINE, PsychInfo, PubMed, Science-Direct, ProQuest Central, and Google Scholar. The initial search was conducted on March 31, 2022, and subsequent searches on March 31, 2023, March 31, 2024, and July 31, 2024. Inclusion criteria were (a) empirical research studies, (b) published in English-language, (c) peer-reviewed journals, (d) involved persons with disabilities, and (e) used CBPR methodology. Keywords, with and without the words disability and disorder, included AIDS, anxiety, attention deficit, autism spectrum, blind, blood disorder, CBPR, cancer, cardiovascular, cerebral palsy, cognitive, cognitive functioning, COVID, deaf, depression, developmental, diabetes, disability, epilepsy, hard of hearing, hearing loss, HIV, hyperactivity, intellectual, kidney/renal condition, mental health, mental illness, multiple sclerosis, muscular dystrophy, neurological conditions, obesity, orthopedic conditions, Parkinson’s disease, physical, pulmonary, schizophrenia, seizure, spinal cord injury, stroke, transition, traumatic brain injury, vision loss, visual, and youth. Exclusion criteria included (a) articles not available in English; (b) studies not conducted in the U.S.; (c) opinions, letters, and news sections; (d) book reviews; (f) insufficient reporting of methodology; and (g) commentaries and editorials. The keyword search yielded 1,549 articles, with one or more keywords appearing in the title or abstract. Of the authors, three individually reviewed each title to determine (a) the study was conducted in the U.S., (b) participants were PWD, and (c) CBPR was identified in the study methodology. This process resulted in 29 articles for further review. Of these, 19 articles met the eligibility criteria.
Data Collection and Abstraction
A systematic review of literature and data collection methods followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021; Tricco et al., 2018). The PRISMA flow chart illustrates this review process (see Figure 1).
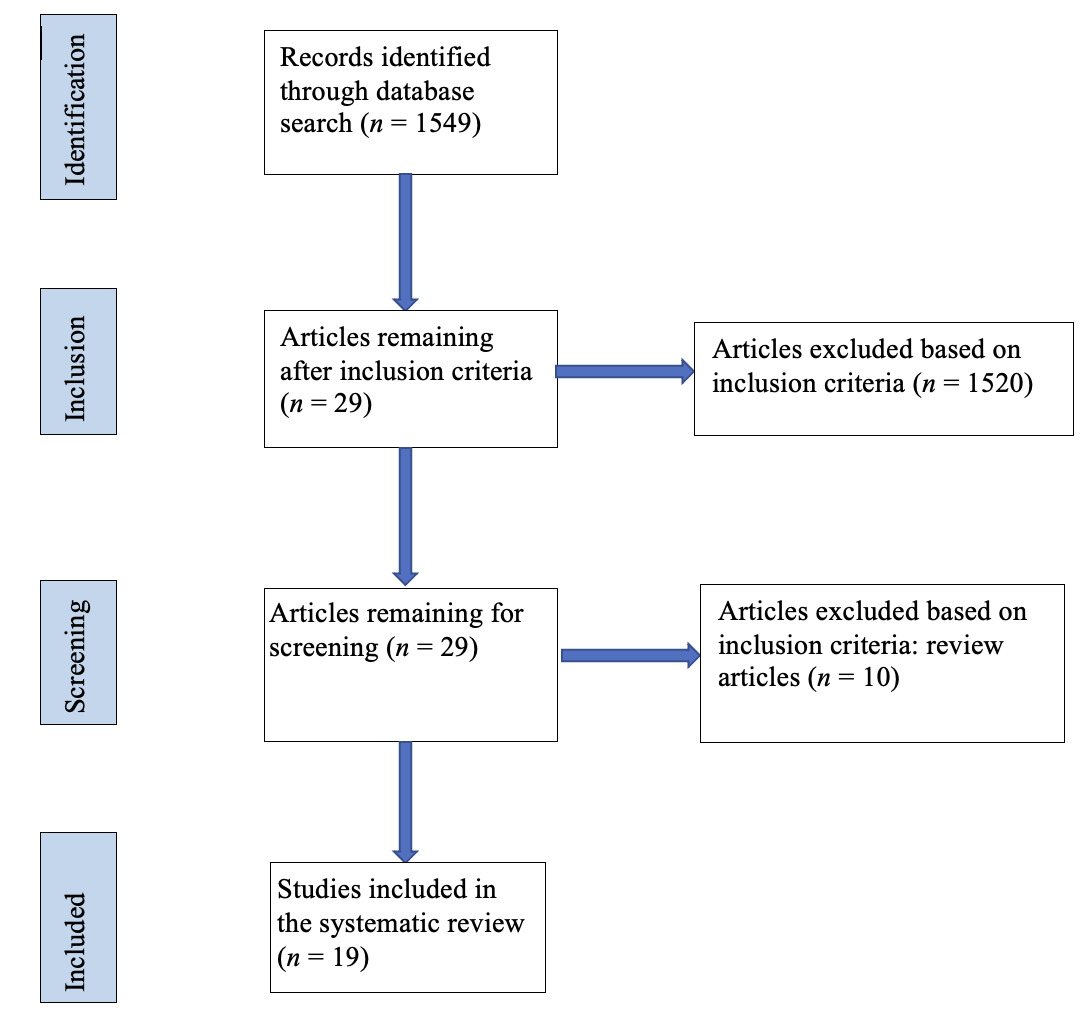
Upon identifying relevant articles, a review process was implemented to determine the feasibility of the literature’s systematic review. To enable this review process, one team member identified articles meeting pre-determined eligibility criteria. Once determined, articles were sent to another team member for verification. Selected articles were sorted based on their relevance to the intended purpose of this review. The final literature search identified 19 studies examining the utility of CBPR to identify and address the priorities of disability communities. Data were abstracted from 19 articles by documenting the identification of each of the six CBPR core components and reviewing them via conventional deductive content analysis. For each article, three authors independently reviewed and reported the study findings within the six CBPR core components. Author discrepancies were addressed, and a consensus was reached. Study data were organized using Microsoft Excel. Cohen’s kappa was reported as .85, suggesting satisfactory interrater reliability (Blackman & Koval, 2000).
Results
Study Characteristics
All (n = 19) studies reviewed were conducted in the U.S. and reported sample sizes (see Table 1). The median number of participants was 30 (range 4–375). Regarding years published, 100.0% (n = 19) were published between 2014 and 2022, of which 36.8% (n = 7) were published within the past five years. Of the studies, disability community was reported as 15.8% (n = 3) African American communities, 15.8% (n = 3) Latino/Latina communities, 5.3% (n = 1) an American Indian community, 5.3% (n = 1) a community of women, 5.3% (n = 1) a community of men, 5.3% (n = 1) a community of young adults, and 5.3% (n = 1) a community of transition age youth. All studies addressed PWD representing 42.1% (n = 8) intellectual and developmental disabilities (IDD), 26.3% (n = 5) mental health (e.g., mental illness, psychiatric disabilities, serious mental health conditions), 10.5% (n = 2) multiple disabilities (e.g., HIV/AIDS and IDD, vision loss and diabetes), 5.3% (n = 1) sensory (e.g., vision loss), 5.3% (n = 1) physical, 5.3% (n = 1) Parkinson’s disease, and 5.3% (n = 1) substance use (e.g., opioid).
CBPR Core Components (see Table 2)
Forming Partnerships
All studies (n =19) reported the process of forming partnerships, suggesting transcendent partnerships in which academics worked with communities to address priorities of mutual interest. Of the studies, 100 % (n = 19) of partnerships included academic researchers, 94.7% (n = 18) included community members, 89.5% (n = 17) included direct service providers, 63.2% (n = 12) included agency personnel, and 15.8% (n = 3) included community leaders.
Assessing Community Strengths and Dynamics
In the studies, assessments were conducted to better understand the needs of the disability community populations inclusive of culture (e.g., race, ethnicity, disability, socioeconomic status, age, immigrant status). Of the studies, 89.5% (n = 17) included the community members in the assessment of community strengths and dynamics, whereas 10.5% (n = 2) reported only academics and direct service providers involved.
Identifying Community Priority Concerns and Research Questions
In all studies (n = 19), partners reported various actions (e.g., reviews of community assessments, interviews, community forums, community meetings, work groups) to identify priorities. This also included governance (e.g., advisory board, advisory council, community advisory board, steering committee) reported in 31.68% (n = 6) of the studies and was composed of academics, direct service providers, and community members.
All studies (n = 19) stated community priorities. Of the studies, 84.2% (n = 16) identified the provision of direct services (e.g., education, health, support, vocational rehabilitation services) and 15.8% (n = 3) of studies identified community member engagement in CBPR (e.g., empowerment, experiences, understanding). Among the priority concern context, 21.1% (n = 4) addressed violence (e.g., abuse, interpersonal violence, awareness) and 15.8% (n = 3) addressed the impact of social issues (e.g., homelessness, poverty, race). Community members were involved in identifying priorities in 89.5% (n = 17) of the studies and the research question in 15.8% (n = 3) of the studies.
Designing and Conducting Etiologic, Intervention, and/or Policy Research
Community members participated in designing and conducting research in 94.7% (n = 18) of the studies. Across studies, CBPR partnership community members were reported as engaged in 101 (M = 6.11, Mdn = 6) research activities. Of these activities, 82.2% (n = 16) of the studies addressed research design (e.g., creating the research design, creating measures, creating content, serving as content experts, developing interview questions, creating structured interviews, developing focus group questions, developing interventions, developing study protocols, ensuring participant comfort and safety). In 21.1% (n = 4) of the studies, community members were involved in participant recruitment (e.g., research participants, partnership members, governance members). Of the studies, 68.4% (n = 13) reported community members involved in conducting the research (e.g., facilitating individual interviews, facilitating group interviews, facilitating focus groups, piloting interventions, piloting surveys, piloting interview guides, survey testing). Community member participation in the data analysis (e.g., data coding, transcript review, theme identification, conducting statistical analyses, conducting thematic analysis) was reported in 84.2% (n = 16) of the studies.
Feeding Back and Interpreting Research Findings
Community members feeding back and interpreting data was reported in 94.7% (n = 18) of the studies. Across studies, community members engaged in activities to ensure findings aligned with and addressed priorities. Of the studies, 68.4% (n = 13) addressed providing data analysis processes feedback (e.g., reviewing data analysis procedures, amending data, describing the data, reviewing data transcripts, reviewing discussion group data, finalizing results) and 52.6% (n = 10) addressed data interpretation (e.g., congruence with community voices, representativeness of community, community approval and consensus).
Disseminating and Translating Research Findings
The translating of research findings to develop products (e.g., peer coaching program for supported education, Sexual Health and Relationship Education model, internet-based Men’s Safer and Stronger Program, Inspiring Change model curriculum, Peer Navigator Program) was reported in 73.7% (n = 14) of the studies. The dissemination of study findings venues (e.g., governance body, professional conferences, newsletter, state agencies, service providers, social service organizations, faith-based organizations, local health care agencies, a multimedia exhibition, community agency providers, websites, rehabilitation administrators, policymakers, parents) was reported in 31.6% (n = 6) of the studies. Several studies, 21.1% (n = 4), reported that study findings informed further research (e.g., a randomized controlled trial, a pilot study, testing of the internet-based Safer and Stronger Program, survey addressing the relationship between violence, disability, and health among people with developmental disabilities).
Discussion
The authors reviewed 19 studies to examine the evidence of the engagement of the disability community in the core components of CBPR. The findings present CBPR as instrumental in creating equitable partnerships among academics (i.e., researchers), agency personnel, direct service providers, and disability community members. Through the CBPR partnership, disability community members were engaged in the research process to identify community priorities and research questions, design and conduct interventions, and translate and disseminate study findings to enhance community well-being. Several findings from this systematic review deserve further discussion.
First, in the reviewed studies, approximately 70% of the community priorities addressed the provision of direct services to PWD. When developing partnerships with researchers and disability communities, the application of the CBPR process presents as beneficial to both when identifying and addressing gaps in service delivery that include the social determinants of health. Within agencies providing direct services (e.g., SDOH), there may be circumstances impacting the quality of services and support that PWD receive. These may include limited financial resources, models that do not account for the quality of services, long waits for service, and high turnover of support staff. Because of these, direct service providers may not be prepared or have the resources to address the needs of persons with disabilities and services may present as non-existent, delayed, incomplete, or of poor quality (American Network of Community Options and Resources, 2014; Iezzoni et al., 2021; Wong et al., 2019). Through CBPR, researchers and direct service providers have the opportunity to partner with disability communities to better understand the service delivery needs (e.g., education, transition services, pre-employment transition services, vocational rehabilitation services) of disability communities from a SDOH perspective and provide technical assistance (e.g., targeted, intensive, universal) to address service delivery challenges and make progress toward equitable services in both local and state education agencies and in state vocational rehabilitation services. When developing CBPR community partnerships, researchers may consider having more than one agency member partner. With one partner per agency, should reorganization occur, that partner may no longer be involved in the CBPR process, resulting in re-establishing the partnership, trust, and commitment to the community priority. The characteristics of promoting partner equity, ongoing dialogue, and power-sharing while negotiating and balancing the interests of partners separates CBPR from the investigator-driven design (Resnik & Kennedy, 2010). Researchers must be aware of potential community-priority identification bias (e.g., funding priorities, programmatic lines of research) and empower communities to identify their own priorities.
Second, when reporting the process for identifying community priorities, less than 33% of the studies reported the use of governance (e.g., advisory board, advisory council, community advisory board, steering committee). Anderson et al. (2021) utilized the CBPR advisory council across all phases (e.g., design, development, implementation, analysis). McDonald & Stack (2016) and Stack and McDonald (2017) reported the use of both a steering committee (SC) and a community advisory board (CAB) in each of the two states. The SCs provided leadership, whereas the CABs provided ongoing guidance to the SCs. Nicolaidis et al. (2015) reported SC roles (e.g., preparing for CAB meetings, monitoring and addressing any concerns with the CBPR process, co-leading CAB meetings) and two state (e.g., Oregon, Montana) CABs roles (e.g., finalize constructs, ensure community priorities, select measures, making recommendations). The use of governance provides an opportunity to have representation of the community, including individuals who are well-known for their community accomplishments. Governance that provides shared leadership and power among community members, academics, agency personnel, and service providers is more likely to sustain the CBPR process. Distinguished from other research approaches, CBPR has the highest level of community involvement and power-sharing as it is not based on who has the funding or power that is driving the research but on how power equity is distributed among the partnership members (Wallerstein & Duran, 2017).
Third, approximately 80% of the studies reported community members as engaged in the research methodology (e.g., identifying the research question, recruitment, data collection, data analyses,). Based upon the research methods considered, CBPR researchers can provide community members the opportunity to explore their method interests and receive training (Israel et al., 2003). Several studies identified community engagement throughout the research process. When exploring the priority of the experiences of race, poverty and disability among African Americans public vocational rehabilitation services, Anderson et al. (2021) reported engaging community members in participant recruitment, focus group facilitation, data analysis, and reviewing findings to ensure representation and accuracy. Corrigan et al. (2020) explored peer coaching in supported education among the community of college and university students with psychiatric disabilities. The student community members were involved in the recruitment process, developing an interview guide, and conducting thematic analyses. To address the priority of housing needs of transition-age youth with serious mental health conditions, Lincoln et al. (2015) reported community members defining the research question, developing interview protocols, facilitating interviews, receiving training in data analysis, and transcribing and coding data. A distinct aspect of CBPR is the engagement of community members throughout the research process to provide invaluable perspectives on community issues, including service provision (Wallerstein et al., 2005).
Fourth, more than 70% of the studies developed products as outcomes of the translation of research findings. CBPR partnerships provide community perspectives from which to develop action and advocacy, translating research findings into probable solutions to address community priority concerns. In the Corrigan et al. (2017) study, the partnership translated the research findings to develop the Peer Navigator Practice (PNP) and procedure manual to address the needs of Latinos with serious mental illness and conduct a randomized controlled trial. Among college and university students with psychiatric disabilities, research findings were translated to create a peer coaching program for supported education (P. W. Corrigan et al., 2020). Research findings addressing the physical abuse and safety needs of men with disabilities were applied to create and evaluate an internet-based Men’s Safer and Stronger program, a program inclusive of the recorded statements, stories, and actions from men with disabilities who were survivors of abuse (Lund et al., 2015). Through CBPR, networks can be created across organizations, agencies, and communities to address community priorities by crossing traditional boundaries, breaking down barriers to services, and enhancing community well-being (Hergenrather et al., 2009).
Fifth, to amplify the utility of the study findings, CBPR includes the dissemination of information in multiple venues and outlets. However, approximately 32% of the studies reported community partners involved in the dissemination of findings. Anderson et al. (2021) reported findings addressing consumer race, disability, and poverty disseminated to policymakers, researchers, vocational rehabilitation (VR) administrators, and VR counselors. Findings addressing direct support and persons with intellectual and developmental disabilities were disseminated to community agency providers and posted on the East Indiana Area Health Education Center website (Auberry, 2016). Corrigan et al. (2017) reported the findings addressing the healthcare needs of Latinos with serious mental illness by disseminating on the ChicagoHealthDisparities.org website. Lincoln et al. (2015) reported the findings addressing young adults living with mental health conditions disseminated to state mental health agencies and direct service providers. Future CBPR studies should involve community members alongside researchers to disseminate findings across multiple outlets, using language that is respectful and understandable to community members.
Sixth, approximately 21% of the studies involved CBPR community members in participant recruitment. Because community members may serve as informal community guides and have access to informal community leaders and networks, they can provide perspectives on community issues that differ from researchers and direct service providers. Corrigan et al. (2015) reported recruitment to include distributing flyers, word of mouth, and a call out to the African American neighborhoods. Corrigan et al. (2020) reported CBPR participant recruitment by using online weekly university news, distributing posters around campus, and emailing students who participated in campus disability center activities. Nicolaidis et al. (2015) reported two community advisory boards, each having four persons with developmental disabilities, recruited CBPR participants via word of mouth, established agreements with state developmental disability agencies, and posted electronic flyers. Because community engagement is essential to the CBPR process, the recruitment process is crucial. Effective CBPR community member recruitment strategies include having the same cultural/ethnic background as the community, being comfortable working with the community, being knowledgeable about the community, and collaborating with trusted organizations. Challenges to community member recruitment include persons not seeing a benefit of involvement, having a poor understanding of what is being studied, lacking knowledge about the topic, and not understanding the time commitment (Bonevski et al., 2014; Vangeepuram et al., 2023).
Finally, approximately 16% of the studies reported community members being involved in identifying the research question. Corrigan et al. (2016) reported that members of the community of Latinos with serious mental illness shared leadership roles in all elements of the research design, which included defining the research questions and hypotheses. Lincoln et al. (2015) reported the research team, inclusive of young adults living with mental health conditions, refined the research question, including the language used. Because the community priority may be based on social inequities and social injustices, community partners should be involved in identifying the research question. Engaging community voices to express concerns empowers a more equitable partnership to reflect their community interests (Kendall et al., 2017; Riccardi et al., 2023).
Limitations
Study findings reported in this systematic review of literature are subject to limitations. First, although a systematic review was conducted, this may not fully represent the applications of CBPR in disability communities as CBPR is a rapidly practice. Second, despite the expansive scope of the search for literature, some articles were likely “missed” or not included because of selected phrasing or timeframe restrictions. Third, although the CBPR process has much potential to provide culturally responsive results, these are contingent upon the academic’s cultural competencies and history of engagement and work within diverse communities. Fourth, among the literature included as part of this systematic review, some components of CBPR were not clearly identified (e.g., dissemination of findings), thus limiting the alignment with the inclusion criteria. Differences among researchers, with regard to the implementation of CBPR, impact the reporting of findings and limit the ability to synthesize information. Fifth, regarding study selection, it is important to acknowledge that even with pre-determined inclusion and exclusion criteria and the use of an interrater process, individual researcher judgement and experience potentially introduce selection and interpretation biases. Finally, the heterogeneity of studies presents as a limitation given the differences in populations, interventions, and outcomes presents difficulty in generalization. . Despite the limitations, this systematic review contributes to disability research by reporting CBPR to combine knowledge and action to create community change.
Conclusion
The systematic review of CBPR explored the engagement of PWD in the CBPR process. The findings present evidence of CBPR as a promising research framework to address disability health disparities and social determinants of health (e.g., education, economic stability). Across the 19 studies, disability communities were engaged in the six CBPR core components. However, CBPR researchers need to be inclusive of disability communities when identifying research questions, creating governance, recruitment, and disseminating findings. We encourage readers of this article to review other CBPR articles to continue learning about CBPR and its applications to disability communities. Given the importance of social equity and reflecting the perspectives of the underrepresented individuals most impacted by research, CBPR provides opportunities for academic researchers to develop community partnerships to empower PWD to engage in action to address disparities and create sustainable community change.