Transition from high school to college can be challenging and stressful, leaving college students particularly vulnerable to alcohol use, illicit substance use, and misuse of prescription drugs. Harmful and underage college drinking are significant public health problems, exacting an enormous toll on the lives of students on campuses across the United States (National Institute on Alcohol Abuse and Alcoholism, 2021). In addition, research indicates problem gambling is associated with alcohol and drug use in college students (Caldeira et al., 2017). The rate of problematic gambling among college students is a concern. Estimates suggest rates are up to five times greater than the general adult population, with 6.13% of college students meeting the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5; American Psychiatric Association, 2013) criteria for gambling disorder (Nowak, 2018). Importantly, empirical evidence suggests gambling disorder and substance use disorder share similar predispositions and personality profiles (Caldeira et al., 2017; Rash et al., 2016; Slutske et al., 2005). Engagement in addictive behaviors has a significant negative impact on physical and mental health and classroom attendance, leading to academic failure (Alexander & Hicks, 2015; Landin & Pérez, 2015). Further, with the proliferation of social casino gaming and gambling, a small body of research shows similar findings between social casino gaming, problematic gambling, drug use, alcohol use, and poor school performance in college students (Petry & Gonzalez-Ibanez, 2015).
The Social Security Administration (SSA) recognizes substance use disorder as a disability category (The Recovery Village, 2021). State vocational rehabilitation agencies also include substance use disorder as a disability and provide psychosocial, educational, and employment services for eligible individuals who recovered from substance use (Rehabilitation Services Administration, 2017). College and university training is an appropriate vocational rehabilitation services for young adults with substance use disorders (Chan et al., 2020; O’Neill et al., 2015). However, it is not sufficient for rehabilitation counselors to merely provide tuition support for young adults who recovered from substance use to attend college. To help with adjustment to college life, academic achievement, and goal persistence, rehabilitation counselors must work with other disability service providers at colleges and universities to provide academic supports (e.g., time management, study skills training, social skills training, health promotion [physical activity and exercise, eat healthily, practice mindfulness meditation and Tai-chi, etc.]), and positive psychological counseling to help college students recovering from substance use disorders develop personal strengths (e.g., hope, resilience, generalized self-efficacy, coping flexibility) and social capital to improve their college life adjustment, academic performance, and goal persistence.
Purpose of the Study
As far as we know, no research exists examining the interactions between SCG, gambling, and substance use in college students and their relationship to college performance indicators such as class attendance. Purpose of this study is to help rehabilitation counselors and disability services providers deliver effective academic and counseling support services for college students recovering from or at risk for substance use disorder and gambling disorder; to help them stop their maladaptive behaviors, adjust positively to college life, and complete college, it is important that we have a better understanding of the effect of social casino gaming, problem gambling, and substance use disorder on class attendance and goal persistence. The aims of this study were to (a) determine the prevalence of social casino gaming, gambling, alcohol use, and drug use in a sample of college students; (b) examine the relationship among social casino gaming, gambling problems, alcohol and drug use, and class attendance; and (c) evaluate the extent to which alcohol and drug use can explain the relationship between gambling problems and class attendance problem.
Methods
Participants
Participants in the present study were 390 undergraduate college students attending a large urban university located in the Mid-Atlantic region who reported social media use. The sample was 55.3% female, with a mean age of 20.72 (SD ± 3.29). For race and ethnicity, 130 participants (36%) were African American/Black, 101 (28%) were European American/White, 55 (15%) were Asian American, 37 (10%) were Hispanic/Latinx, and 38 (11%) were other. As for disability status, 118 participants (21.8%) identified as having a disability. Of those, 32 participants (27.1%) reported a mental health condition, followed by a sensory condition (n = 31, 26.3%), a learning disability (n = 30, 25.4%), a mobility condition (n = 10, 8.5%), and substance-related and addictive disorders (n=5, 4.2%). The four undergraduate classes had a balanced representation. Demographics of participants are presented in Table 1.
Measures
Social Casino Gaming
Social casino gaming was assessed by the question, “Have you ever played a social media casino game (such as Bingo Bash, Double Down Casino, Texas Hold’em, and Poker Lucky Slot, etc.)?” This item is rated on a dichotomous scale with 0 (No) and 1 (Yes).
Gambling
The Problem Gambling Severity Index (PGSI), developed by Ferris and Wynne (2001), was used to assess gambling problems. It is a 9-item measure (e.g., “Have you bet more than you could really afford to lose?”). Each item is rated on a four-point Likert-type scale, ranging from 0 (never) to 3 (almost always). Scores are calculated by summing the PGSI items. The total range is from a minimum 0 to maximum 27, with a score of 0 indicating no gambling problem, score of 1 or 2 indicating low level of problems with few or no identified negative consequences, score of 3 to 7 indicating moderate level of problems leading to some negative consequences, and a score of 8 or more indicating problem gambling with negative consequences and a possible loss of control. The PGSI is a unidimensional scale with good internal consistency reliability (Cronbach’s alpha > .85) and construct validity (Holtgraves, 2009; McMillen & Wenzel, 2006; Miller et al., 2013). In the present study, Cronbach’s alpha was computed to be .93.
Alcohol Use
The Alcohol Use Disorders Identification Test (AUDIT) was developed by the World Health Organization (WHO) to assess alcohol consumption, drinking behaviors, and alcohol-related problems (Saunders et al., 1993). It is a 10-item screening measure (e.g., “How often do you have a drink containing alcohol?”). Each item is rated on a five-point Likert-type scale [e.g., 0 (never) to 4 (daily or almost daily)] or a three-point Likert-type scale [e.g., 0 (no), 2 (yes, but not in the last year), 4 (yes, during the last year)]. Scores are calculated by summing the items. The total range is from minimum 0 to maximum 40, with a score of 8 or more indicating hazardous or harmful alcohol use. The AUDIT has good reliability (.80), and concurrent and construct validity (De Meneses-Gaya et al., 2009). In the present study, Cronbach’s alpha was computed to be .76.
Drug Use
Cut Down, Annoyed, Guilty, Eye-opener (CAGE) – Adapted to Include Drugs (CAGE-AID; Brown & Rounds, 1995) was used to assess potential problems with drug use. This measure is adapted from the original screening instrument for alcohol use (Mayfield et al., 1974). It is a 4-item measure (e.g., “Have you ever felt you needed to cut down on your drinking?”). Each item is rated on a dichotomous scale with 0 (No) and 1 (Yes). Scores are calculated by summing the items. The total score ranges from minimum 0 to maximum 4, with a total score of two or greater is considered clinically significant. The CAGE-AID has been independently validated, and results indicated that it has high reliability (.92) and construct and concurrent validity (Basu et al., 2016; Leonardson et al., 2005). In the present study, Cronbach’s alpha was computed to be .70.
Class Attendance Problem
Class attendance problem was assessed by a question “How often would you say you miss class?” It was answered 1 (never), 2 (once a semester), 3 (once a month), 4 (more than once a month), 5 (once a week), and 6 (more than once a week).
Procedure
After receiving institutional research board approval, data were collected from a large urban university located in the Mid-Atlantic region of the United States. Students were recruited through flyers that were distributed throughout the campus and residence halls. Students were eligible to participate if they met the following inclusion criteria: (a) a student at the university; (b) 18 years and older; and (c) played any type of social media game within the past week. The survey took between 25-45 minutes to complete. Once completed, participants were compensated with a $20 gift card.
Data Analysis
Descriptive statistics and correlational analyses were computed using the Statistical Package for the Social Sciences (SPSS, version 26.0). In addition, two formulas were used to correct for attenuation, one for Pearson correlations (Spearman, 1904; Trafimow, 2016) and one for point-biserial correlations (Becker, 1986). Correction for attenuation is a statistical process developed by Charles Spearman in 1904 to correct the weakening effect of measurement error on correlation coefficients (Jensen, 1998). The PROCESS macro, written by Hayes (2017), was used to estimate the total, direct, and indirect effects of gambling problems on class attendance problem through the alcohol and drug use problem variables.
Results
Descriptive Statistics
The prevalence of social casino gaming, gambling, alcohol use, drug use, and attendance problem were computed using descriptive statistics. Means and standard deviations for the clinical assessment instruments are presented in Table 2. Sixty-one students in this study (15.64%) reported they have experience playing social casino gaming. The mean rating for the gaming problem was 0.16 (SD = 0.36). In terms of the gambling problem, 36 students (9.23%) indicated they have some gambling problems, and eight students (2.05%) can be diagnosed as having clinically significant gambling problems (PGSI scores > 7). The mean rating for alcohol use problems was 4.11(SD = 5.38), and 78 participants (20.5%) showed hazardous or harmful alcohol use (AUDIT scores > 7). The mean rating for the drug use problem was 0.41 (SD = 1.11), and 47 students (12%) were considered to have a clinically significant level of drug use (a total score of two or greater). One hundred and nine (28%) students missed classes at least once a week.
Correlation Analysis
The reliability of the clinical measure instruments varies significantly, with PGSI having the highest reliability coefficient of .93 and the reliability coefficients for AUDIT (.76) and CAGE (.70) in the acceptable range. However, the correlation between the two measures is affected by the reliability of each measure. Spearman (1904) proposed the correlation between two measures should be attenuated as if the scores on both measures had perfect reliability to reveal the true relationship of the two constructs.
Correction for Attenuation
Attenuation is a statistical concept that refers to underestimating the correlation between two different measures because of measurement error (Spearman, 1904). Correction for attenuation developed by Spearman is a statistical procedure to estimate the correlation between two measures, if the scores on both had perfect reliability. In the present study, we used two formulas to correct for attenuation.
Pearson correlations: Rxy=rxy/√reliabilityx reliabilityy
Point-biserial correlations: rc=r/√r2+4pq(1−r)2
After correction for attenuation, the magnitude of the significant correlations increased appreciably, with correlations ranging from .20 to .38 (low to moderate-high effect sizes). Social casino gaming was significantly associated with problem gambling (r = .38, p < .01) and drug use problem (r = .27, p < .01), but not with class attendance problem (r = .03, p = .30, n.s.). Gambling problem was related to alcohol use problem (r = .20, p < .01) and drug use problem (r = .24, p < .01), but not with class attendance problem (r = -.01, p = .67, n.s.). Alcohol use was related to drug use (r = .30, p < .01) and class attendance problem (r = .24, p < .01). Drug use was not related to attendance (r = .09, p =.07). The significant attenuated correlations ranged from .15 to .38. The effect size is low if the value of r varies around 0.1, medium if r varies around 0.3, and large if r varies more than 0.5. Correlations before and after correction for attenuation and effect sizes are presented in Table 3.
Findings of the correlation analysis suggest that social casino gaming is associated with gambling problems, gambling problem is positively related to alcohol use and drug use problems, and alcohol and drug use were related to attendance problem. It appears that gambling problem affects class attendance problem indirectly through alcohol use and drug use. We tested these indirect effects between gambling problems and class attendance problem through a parallel mediation model.
Mediation Analysis
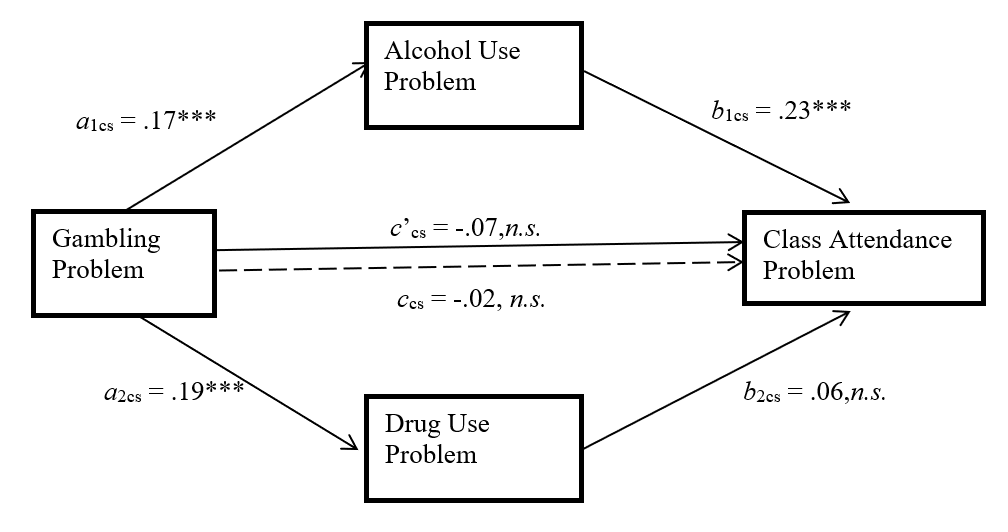
As indicated by Hayes (2017), since correlation between X and Y does not determine the size of mediation effect, significance of total effect is not a requisite condition for proceeding with mediation analysis. More specifically, tests of significance for the individual paths a (from independent variable (X) to a mediator (M)) and b (from M to dependent variable (Y)) are not required to determine whether M mediates the effect of X on Y (Hayes, 2017). Therefore, we conducted a parallel mediation analysis to test the hypothesis that the gambling problem has an indirect effect on classroom attendance through alcohol use and drug use. The mediation results indicated that the gambling problem was not associated with class attendance problem (total effect: ccs = -.02, p = .67). Gambling problem was a significant predictor of alcohol use problem, a1cs = .17, p< .001, and drug use problem, a2cs = .19, p< .001. Alcohol use problem was a significant predictor of class attendance problem, b1cs = .23, p< .001, after controlling for the effect of gambling problem and drug use problem. Although drug use problem was significantly related to gambling problems and alcohol use problems at the bivariate correlation level, it is not a significant predictor of class attendance problem after controlling for the effect of a gambling problem and alcohol use problem, b2cs = .06, p = .28. Gambling problems did not have a direct association with class attendance. However, it had a significant indirect effect on class attendance problem through alcohol use problems and drug use problems (direct effect: c’ = -.07, p = .16, n.s.). The indirect effect was tested using a bootstrap estimation approach with 5,000 samples (Hayes, 2017). These results indicated only one indirect effect coefficient was significant (a1b1= .04, 95% CI = .004, .050), supporting the association between gambling problem and class attendance problem through alcohol use problem. The indirect effect of gambling on class attendance through drug use was not significant after controlling the effect of alcohol use. A graphical presentation of the parallel mediation model for class attendance problem and information for the path coefficients (a1cs, a2cs,b1cs, b2cs, ccs, and c’cs) is presented in Figure 1.

Discussion
Findings of the present study indicate the prevalence rates of social casino gaming, problem gambling, alcohol use, and drug use are similar to the prevalence rates reported in similar studies (Dussault et al., 2017; Nowak, 2018; Veselka et al., 2018). In the present study, social casino gaming was significantly associated with problem gambling (r = .38, p < 01; medium effect size) and drug use (r = .27, p < 01; close to medium effect size). Although social casino gaming is not considered real gambling, there is an overlap between these two activities, and research has indicated that social casino gaming is related to gambling and gambling severity (Gainsbury et al., 2014, 2017; King et al., 2014). In a population of college students, Caldeira et al. (2017) found that gambling and substance use shared the same risk factors. It is possible that it applies to SCG as well. This hypothesis requires further research, however, it already has some indirect support in findings that SCG players willing to do micro-transactions are more at risk of gambling (Gainsbury et al., 2016; Kim et al., 2015) and are more impulsive and sensitive to reward compared to non-paying SCG players (Kim et al., 2017). Impulsivity is considered an early risk factor for the development of gambling problems (Dowling et al., 2015). It should be noted that both social casino gaming and problem gambling were not associated with class attendance. This finding is contrary to previous research reporting that problem gambling is related to class attendance problem (Petry & Gonzalez-Ibanez, 2015) and poor academic performance (Potenza et al., 2011). This discrepancy of our findings and previous research could be explained by a small number of gamblers in our sample. Alcohol use and drug use were negatively and significantly associated with class attendance. The participation in alcohol and drug use in college students’ populations has been shown to have a negative impact on school performance (Arria et al., 2017; Kelly et al., 2015; Palmer et al., 2012). Decreased school attendance has been associated with increased substance use and may be an indicator of disengagement from school and other school related problems (Hemphill et al., 2014; Heradstveit et al., 2017).
The correlations among social casino gaming, problem gambling, drug use, alcohol use, and class attendance reveal an interesting pattern. There are no direct relationships between social casino gaming, problem gambling, and class attendance problem. The association between social casino gaming/problem gambling and class attendance problem can only be explained through alcohol use and drug use. While drug use was found to correlate with class attendance problem at the bivariate correlation level, it was not a significant mediator after controlling for the effect of gambling problems and alcohol use problems. The parallel mediation analysis confirmed students at risk for gambling problems were more likely to have alcohol use problems, and alcohol use problems led to poor class attendance. The interplay of gambling and substance use is well documented (Caldeira et al., 2017; Geisner et al., 2016; Loo et al., 2019; Sharman et al., 2019; Tackett et al., 2017) and our study contributes to previous findings that this is also the case for SCG (Gainsbury et al., 2014). Our results show that these activities, especially in combination, are directly or indirectly related to poorer participation in classes among college students.
Implications
Findings from this study indicate that SCG can lead to gambling problems. Furthermore, engagement in SCG and gambling can contribute to hazardous and harmful substance use, causing disruptions in class attendance and potentially exacerbating academic-related problems. As missed classes are a risk factor for poor academic performance and drop out, this study supports college-wide prevention and early intervention programs to improve academic outcomes. Research has shown that these problems are often initiated in high school (Arria et al., 2008, 2017; Dussault et al., 2017), thus efforts to correct faulty beliefs about the normative nature of these activities should begin early (Arria et al., 2017).
Rehabilitation counselors and disability services providers who work with college students must be mindful of the relationship between social casino gaming, gambling problem, drug and alcohol use problem, and class attendance, as well as the consequences of addictive behaviors on physical health, mental health, and academic performance (Arria et al., 2017; Caldeira et al., 2017; Kelly et al., 2015; Martens et al., 2009; Martin et al., 2014; Petry & Gonzalez-Ibanez, 2015). Assessment of these addictive behaviors must be included in the assessment battery of rehabilitation counselors and other disability service providers who work with college students with or without disabilities. When absence from class and worsening academic performance is present, the underlying reasons must be identified. While students presenting with attendance issues should be screened for alcohol and/or drug use problems, it is critical to assess for often overlooked behaviors, such as social casino gaming and gambling.
For counselors working with students with addiction issues, research has indicated the potential for using positive psychology interventions to treat gambling, alcohol, and drug use problems (Krentzman, 2013; Scharff, 2014). Brief interventions, such as personalized feedback, have also been effective in reducing addictive behaviors in the student population, especially in low to moderate severity and in the short-term perspective (Gulliver et al., 2015; Jeffries et al., 2016; Martens et al., 2015). Moreover, findings of this study have implications beyond the college student population. There are empirical studies that indicate because of social isolation and social distancing, online gambling soared during the COVID-19 pandemic (Cataldo et al., 2022; Price, 2020). Therefore, it may be cogent for counselors to include the PGSI, AUDIT, and CAGE as part of their intake assessment battery.
Future research should further explore the relationships between SCG, gambling, and substance use, and their impact on academic performance in more detail. This study clearly showed that there was an association among the examined variables, but future studies could examine the degree of severity of SCG and how it is related to gambling, as well as to class attendance and outcomes. The new instrument, Problematic Social Casino Gaming Scale developed by Li et al. (2020), could be used for this purpose.
Limitations
There are several limitations of the study that need to be mentioned. This study was conducted at a large publicly funded, urban university. Thus, results may not be generalizable to students in other types of colleges and universities in other areas. The numbers of participants with problem behaviors (i.e., gambling problem, alcohol use, drug use) were small (about 10% of the sample), so the results must be considered with caution. We use a one-item measure to assess social casino gaming and a one-item measure for classroom attendance. Both are self-report measures, which could introduce social desirability biases. Therefore, it might have led to results that are inconsistent with the literature. Future research should develop and validate a lengthier measure to better quantify these constructs. Several relevant measures, such as social isolation, depression and anxiety, global health, and goal persistence, should be included in future studies to provide a complete picture of the impact of gambling problems, alcohol use, and drug use on physical health, mental health, academic performance, and goal persistence of college students with or without disabilities.