More than 87 million confirmed cases of COVID-19 and more than 1 million related deaths have been confirmed in the United States since the first case was reported in January 2020 (Centers for Disease Control and Prevention, n.d.-a). In March 2020, the CDC (n.d.-b) provided COVID-19 guidance, including social distancing protocols, preventative measures, and information about variants and vaccine roll-out. They also reported that persons with disabilities (PWD) were at higher risk for contracting COVID-19 than those without disabilities “because of underlying medical conditions, congregate living settings, or systemic health and social inequities” (Centers for Disease Control and Prevention, n.d.-c, para. 2). In the U.S., PWD are considered the largest minorized group, representing approximately 26% of the population (Lund et al., 2020) and experience adverse events, such as a pandemic (e.g., COVID-19, financial recession) or natural disaster (e.g., hurricane, flooding, earthquake), in a unique manner that often causes undue stress and trauma, potentially triggering life-altering decisions (e.g., to continue attendant care; Lund et al., 2020).
For example, persons with multiple sclerosis (MS) experience a range of physical and cognitive impairments, increasing psychological distress, but little research explores disability-related stressors and proper coping strategies (Cerea et al., 2021). Among PWD, persons with MS reported experiencing employment-related concerns due to a higher risk of contracting COVID-19 than the general population (Bishop & Rumrill, 2021; Moss et al., 2020). However, there is limited published research addressing how the stress and trauma from such events present as barriers to health care, employment, earning capacity, and educational attainments for PWD compared to those without disabilities (Moen et al., 2020; Rotarou et al., 2021). In June 2020, the National Bureau of Economic Research officially declared the United States in an economic recession as a result of COVID-19, further impacting available employment opportunities for many individuals with and without disabilities (Schall et al., 2021) and creating increased financial stressors for PWD (Global Disability Inclusion, 2020).
COVID-19 presented disruptions to work routines and unprecedented job loss for millions of people, including PWD (McAlpine & Alang, 2020; Moen et al., 2020; A. E. Schwartz et al., 2021). During COVID-19, several industries and businesses reported reducing their number of employees, decreasing services, reorganizing the workplace environment from in-person to virtual or closing, and providing individuals hired in entry-level employment with limited employment opportunities (e.g., reduced hours, termination, working from home; Schall et al., 2021; Sheppard-Jones, Avellone, et al., 2021). Many employment service organizations that provided support to persons with significant disabilities (e.g., supported employment services, customized employment services) reported significantly reduced or removed service provision, therefore decreasing access to services needed to gain and maintain employment (Schall et al., 2021).
Kerr et al. (2012) reported that a “complex relationship exists” between stressors of an individual’s environment (e.g., unemployment) and the use of an appropriate coping mechanism, noting that many typical methods potentially increase stress levels in certain circumstances (p. 280). Because of COVID-19, PWD reported changes in their daily work routines (e.g., moved from in-person to remote work), experienced difficulty accessing medical services, and reported increased mental health-related concerns resulting from inaccessibility or social isolation (Okoro et al., 2021; A. E. Schwartz et al., 2021). Throughout COVID-19, PWD have reported increased mental health challenges due to fear of contracting the virus, increased social isolation, fear of job loss, lack of support, fear of discrimination, and increased anxieties related to their ability to access health care (Bishop & Rumrill, 2021; Sheppard-Jones, Avellone, et al., 2021; Umucu, Tansey, et al., 2021). For example, among PWD, persons with multiple sclerosis and other chronic conditions reported greater social isolation and withdrawal because of COVID-19 social distancing and quarantine protocols (Koch et al., 2021).
Research suggests PWD often encounter barriers to employment (e.g., discrimination, inaccessibility of accommodations; Adams et al., 2021). The Americans with Disabilities Act (ADA) and the Workforce Innovation and Opportunity Act (WIOA) presented federal legislation to increase inclusive opportunities for PWD for integrated, competitive employment and accessible healthcare facilities or equipment (Henry, 1989; Lund et al., 2020). Despite federal legislation to reduce discrimination or integrated supportive services that include vocational rehabilitation (VR), PWD continue to experience significant barriers and disparities in their environments, including social (e.g., stigma, discrimination), policy, physical, environmental, attitudinal, and employment (Baker et al., 2018; Dutta et al., 2008; Sundar et al., 2018).
As PWD experience barriers and disparities in accessing inclusive employment options, a disparate employment gap exists between working-age PWD and working-age persons without disabilities (Baker et al., 2018). In October 2020, the employment rate for working-age PWD was recorded at 33.5%, compared to the employment rate for working-age persons without disabilities at 76.0% (Office of Disability Employment Policy, 2021). In October 2021, there was a 36.8% employment rate for working-age PWDs compared to 76.6% for working-age persons without disabilities (Office of Disability Employment Policy, 2021). Among PWD, individuals with intellectual or developmental disabilities have experienced increased rates of job loss due to the reduction of entry-level positions during periods of economic stress and loss of on-site employment support (Rosencrans et al., 2021; Schall et al., 2021; Sheppard-Jones, Goldstein, et al., 2021).
For PWD, employment provides a sense of purpose, a sense of identity, opportunities for growth, and an increased ability to address change (Dutta et al., 2008; Graham et al., 2018; Saunders & Nedelec, 2014). PWD, compared to employed persons who experience long-term unemployment, are at a greater risk of mental health concerns (e.g., anxiety, depression, substance use; Graham et al., 2018; Sprong et al., 2019). Prolonged unemployment for PWD has been reported as a trigger for chronic stress, often leading to adverse effects on mental and physical health (Kerr et al., 2012).
Purpose
For PWD, COVID-19 presented an adverse event that impacted employment status, support services, and quality of life. The World Health Organization (WHO, 2012) defines quality of life as “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns” (para. 1). To understand better the experiences of PWD during the COVID-19 pandemic in the U.S. and to better serve PWD through future adverse events, a systematic review of literature was conducted to explore the impact of COVID-19 on the lives of PWD. The objectives for this systematic review of literature are to explore the published literature to better understand the effects of COVID-19 on the employment status, support services, and quality of life of PWD during COVID-19.
Methods
Review Process
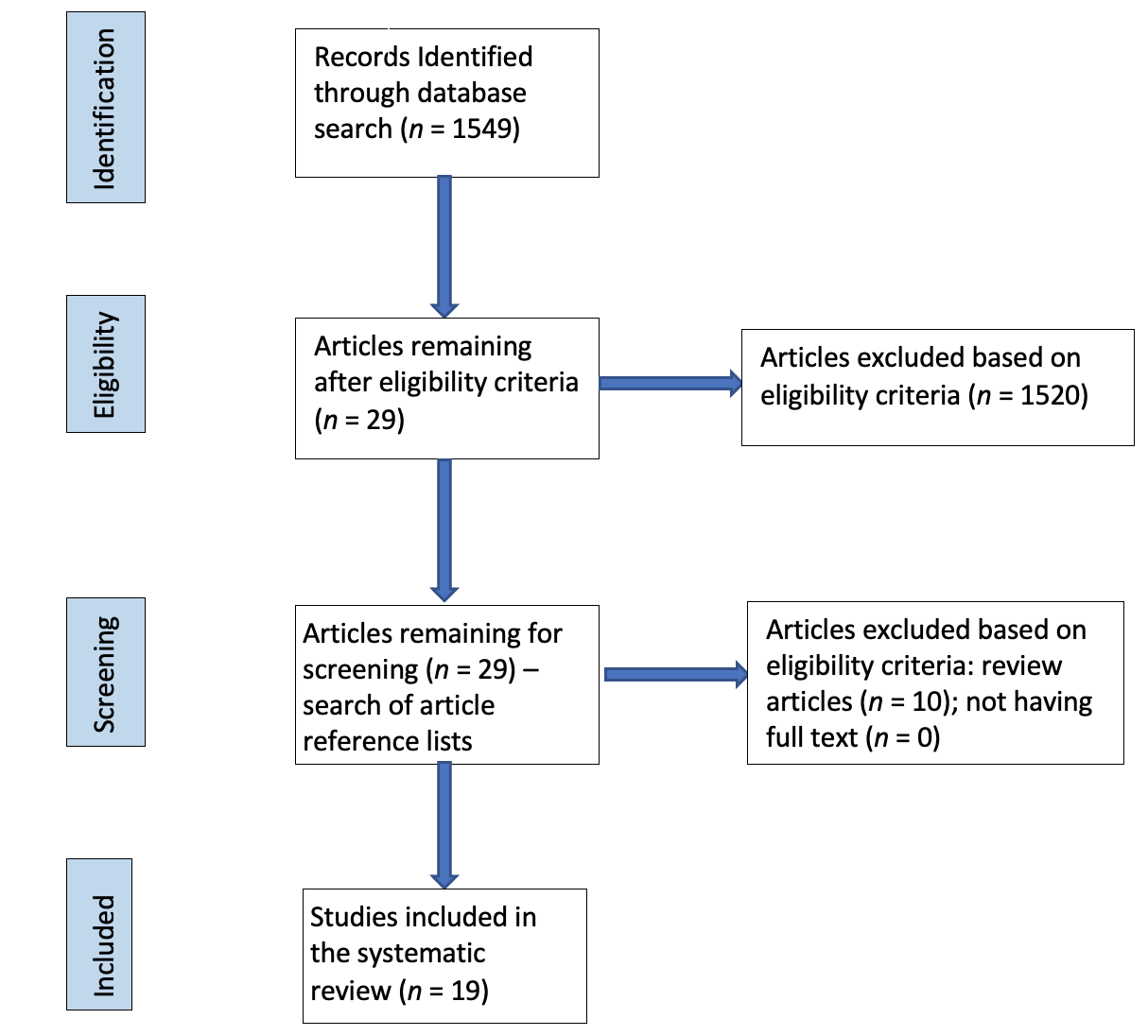
This systematic review of the literature, conducted by authors who had experience working in state vocational rehabilitation services, included a search of online databases to retrieve information on both electronic and paper copies of published articles from January 2020 through December 2021. A database search was facilitated using EBSCO, MEDLINE, PsychInfo, PubMed, Science-Direct, ProQuest Central, and Google Scholar. The initial search was conducted on March 10, 2021; updates were conducted on May 18, 2021, November 17, 2021, and January 14, 2022. Based on the final database search, the authors agreed that since no additional articles were found during this search, it would be best to present the information to ensure reviewed articles remain relevant. Using keywords, each database was searched from inception through January 2022. Keywords included COVID, COVID-19, coronavirus, pandemic, vocational rehabilitation, job, employment, unemployment, disability, chronic illness, job loss, re-employment, remote, retired, urban, rural, telework, telehealth, isolation, depression, loneliness, social support, anxiety, stress, mental health, and counseling. Keywords were selected by the authors based on the purpose of this systematic review of literature and common barriers experienced by PWD. Exclusion criteria were (a) articles not available in English; (b) commentaries and editorials; (c) opinions, letters, and news sections; (d) book reviews; (f) insufficient reporting of methodology or results; and (g) articles not published in the United States. The initial keyword search yielded more than 1,500 articles, with one or more keywords appearing in the title or abstract. Authors individually reviewed each title to determine if (a) the study was conducted in the U.S.; (b) participants were adults with disabilities, eligible to receive VR services; (c) at least one dependent variable was health-related; (d) at least one independent variable related to employment outcomes; and (e) the study focused on the impact of COVID-19. This process resulted in 29 articles for further review. Of these, 19 articles met eligibility criteria by reporting the impact of COVID-19 on areas of employment, quality of life, and coping for PWD.
Data Collection and Abstraction
A systematic review of literature and data collection methods followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021; Tricco et al., 2018). The PRISMA flow chart (see Figure 1) illustrates this review’s search and inclusion process.

Upon identifying relevant articles, a review process was implemented to determine the feasibility of the literature’s systematic review. To enable this review process, one team member identified articles meeting pre-determined eligibility criteria. Once articles were determined, they were sent to another team member for verification. Selected articles were sorted based on their relevance to the intended purpose of this review in areas of impact on employment, quality of life, and coping. The final literature search identified 15 quantitative and four qualitative studies examining the impact of COVID-19 on employment for PWD within the United States. To address interrater reliability of the data abstraction, authors measured interrater reliability after they independently organized the studies by reviewing identified themes and the grouping of related articles. Cohen’s kappa was reported as .85, suggesting satisfactory interrater reliability (Blackman & Koval, 2000).
Results
Study Characteristics
Of the 19 studies reviewed, 100% were conducted in the United States, of which 78.9% (n = 15) were quantitative and 21.1% (n = 4) were qualitative. Sample sizes were reported for all studies. The mean number of participants for studies (n = 19) was 691.5 (Mdn = 269, range: 14-5,119). Of the studies 26.3% (n = 5) reported 14 to 69 participants, 52.6% (n = 10) reported 119 to 404 participants, and 21.1% (n = 4) reported 1,004 to 5,119 participants. All studies were published in 2020 or 2021. The majority of studies, 84.2% (n =16), were published in 2021 (see Table 1).
Participant gender was presented in 100.0% (n = 19) of the studies, of which 15.8% (n = 3) reported gender as being predominantly “men” or “male”; 21.1% (n = 4) reported gender as being predominantly “women” or “female”; 36.8% (n = 7) reported gender as “male and female” or “men and women”; and 26.3% (n = 5) reported gender-inclusive of “non-binary,” “transgender,” “gender-queer,” or another gender identity. Among the identified studies, 63.2% (n = 12) reported participant race/ethnicity (e.g., Asian, Native American, Black, White, Hispanic or Latinx, or other); 21.1% (n = 4) reported race/ethnicity verbally (e.g., “majority of participants were”); and 15.8% (n = 3) did not report race/ethnicity as part of the data collection. The sample mean age of the participants was reported in 52.6% (n = 10) of the studies, of which 30.0% (n = 3) reported age and 70.0% (n = 7) reported an age range (e.g., 18 or more years of age).
All research studies were inclusive of PWD. Of the studies 47.4% (n = 9) reported disability inclusively and descriptively (e.g., cognitive/learning limitations, physical limitations, speech/language impairment, blindness/visual Impairment); 15.8% (n = 3) reported disability in general (e.g., collective disability, chronic illness); 15.8% (n = 3) reported on individuals with multiple sclerosis (MS); 10.5% (n = 2) reported on individuals with intellectual and developmental disabilities; 5.3% (n = 1) reported on individuals with traumatic brain injury (TBI); and 5.3% (n = 1) reported on individuals with a spinal cord injury (SCI).
Several measures were utilized to measure the impact of COVID-19. Of the studies, 42.1% (n = 8) reported an author-created scale to assess or measure health behaviors (Bishop & Rumrill, 2021; Czeisler et al., 2021; Moss et al., 2020; Rosencrans et al., 2021), attitudes toward COVID-19 (e.g., COVID-19 Negative Attitudes Scale; Umucu, Reyes, et al., 2021), effects of COVID-19 on employment (Morrow et al., 2021), engagement in social media (Dobransky & Hargittai, 2021), quality of life (Okyere et al., 2021), and use of services (A. E. Schwartz et al., 2021).
Of the studies, 36.8% (n = 7) utilized standardized measures to assess the impact of COVID-19 associated with character strengths (Global Assessment of Character Strengths-24; GACS-24), coping (Brief COPE), experiences (Scale of Positive and Negative Experience; SPANE), functional limitations (World Health Organization Assessment Schedule II; WHODAS 2.0), loneliness (Positive emotion, Engagement, Relationships, Meaning, and Accomplishment -Profiler; PERMA-Profiler), mental health (Patient Health Questionnaire-4; [PHQ-4], Patient Health Questionnaire-8 Screener [PHQ-8], Hospital Anxiety and Depression Scale; HADS), resilience (Brief Resilience Scale; [BRS], Connor-Davidson Resilience Scale; CD-RISC), stress (Perceived Stress Questionnaire-8; [PSQ-8], Perceived Stress Questionnaire; PSQ), and well-being (PERMA-Profiler, Flourishing Scale; FS). Among reviewed studies, 21.1% (n = 4) reported semi-structured interview protocols (Adams et al., 2021; Cochran, 2020; Epstein et al., 2021; Okyere et al., 2021), and 5.3% (n = 1) used employment services records (Schall et al., 2021).
Quantitative methodology was reported in 75% (n = 15) of the studies and consisted of 40.0% (n = 6) regression analysis (e.g., hierarchical logistic regression, logistic regression, mediation analysis, moderation analysis, ordinary least squares regression), 20.0% (n = 3) chi-square analysis, and 13.33% (n = 2) using prevalence estimates. Qualitative methodology was reported in 21.1% (n = 4) of the studies that included focus groups (n =2), phone interviews (n = 1), and a cross-sectional survey (n = 1).
Review of Findings
The review presented three common groupings identified as employment (e.g., job status, support services), quality of life (e.g., COVID-19 information, health, COVID-19 testing), and coping (e.g., stress, adjustment).
Employment
The relationship between employment and COVID-19 was reported in 63.2% (n = 12) of the studies reviewed. The employment grouping consisted of two themes identified as job-status and support services. Of the studies, 42.1% (n = 8) reported the association between COVID-19 and job status. COVID-19 was associated with higher job loss rates and other work changes (e.g., working fewer hours, transitioning to remote work). Additionally, COVID-19 negatively impacted employment in specific job industries (e.g., food service, health care, hospitality, retail), disability types (e.g., TBI, MS), and among individuals with lower levels of education (e.g., high school diploma, less than a four-year college degree). A few studies (n = 4) reported a relationship between COVID-19 and support services delivery. COVID-19 was reported to impact the availability of support services (e.g., no longer available, inconsistent delivery) and those services for specific disability types (e.g., MS, I/DD).
Quality of Life
The relationship between an individual’s perceived quality of life and COVID-19 was reported in 47.4% (n = 9) of the studies. The quality of life grouping consisted of three themes identified as COVID-19 information, health status, and COVID-19 testing. Of the studies, 15.8% (n = 3) reported a relationship between quality of life and COVID-19 information. Quality of life was associated with inaccessible COVID-19 information, use of social media to exchange information, and disruptions in service provider communication (e.g., service delays, service cancellations). A few studies (n = 4) reported an association between COVID-19 and health status. COVID-19 was positively correlated with increased rates of self-reported mental health concerns (e.g., anxiety, depression, suicidal ideation, substance use), a higher number of individuals self-reporting physical health concerns (e.g., pain, mobility), and an increased frequency of self-reported diagnostic impressions (e.g., less positive feelings, increased irritability, lack of joy, isolation). Two studies reported an association between quality of life and COVID-19 testing (e.g., access to, results). PWD reported difficulties accessing COVID-19 testing sites and concerns about what positive results would mean in regard to living arrangements for self and others (e.g., residence/household members, family).
Coping
The association between coping and COVID-19 was reported in 36.8% (n = 7) of the studies. The coping grouping consisted of two themes identified as stress and COVID-19 survival. Of the studies, 21.1% (n = 4) reported the relationship between COVID-19 and stress. Among PWD, survival during COVID-19 presented higher levels of stress and worry (e.g., job loss, housing stability, access to health care) and lower levels of well-being. A few studies (n = 3) reported a relationship between COVID-19 and COVID-19 survival. Coping during COVID-19 was positively correlated with increased use of substances, behavioral impressions (e.g., avoidance, denial, self-blame), religion/faith (e.g., beliefs, practices), and character strengths (e.g., wisdom and knowledge, courage, humanity, justice, temperance, transcendence).
Discussion
COVID-19 presented significant challenges for individuals with and without disabilities and is often referred to as “unprecedented times.” PWD experienced exceptional stress levels due to various environmental changes, often being left without support or guidance on coping strategies (Umucu & Lee, 2020). The authors presented a systematic review of 19 published studies to summarize what is known about the impact of COVID-19 on PWD. Based on the systematic review, the findings suggest that COVID-19 had a negative impact in areas of employment, quality of life, and coping for PWD. Several findings from this systematic review deserve further discussion.
First, within the grouping of employment, the relationship between COVID-19 and both job status and access to support services was reported across several studies. Because of COVID-19, people with disabilities reported changes in job status (e.g., higher job loss rates, fewer hours employed, working remotely) and changes in support service status (e.g., no longer available, inconsistent availability). PWD, compared to persons without disabilities, are less likely to have completed a bachelor’s degree, are more likely to be employed part-time, and more likely to work in service, production, transportation, material moving, sales, and office occupations (U.S. Bureau of Labor Statistics, 2022). During the early months of COVID-19 in the U.S., many retail and restaurant businesses were among the first to reduce their labor force, thus impacting the job status of PWD (Sheppard-Jones, Avellone, et al., 2021). Sinclair et al. (2020) reported that individuals with intellectual disabilities reported changes in employment status (e.g., reduced hours employed, job loss) due to COVID-19. Throughout the months of February 2020 through January 2021, PWD experienced job status changes that included transitioning from being employed to becoming unemployed, temporary layoffs, and termination (Houtenville et al., 2021). During the COVID-19 pandemic, PWD, compared to persons without disabilities, experienced adjustments in their workforce engagement (e.g., access to technology, remote work, implementation of safety measures) and greater job loss rates (Jashinsky et al., 2021).
During COVID-19, PWD reported changes in the availability status of support services (e.g., personal attendant care, medical care, employment-related services), which were impacted by social distancing protocols (Na & Yang, 2022). Persons with PWD often utilize support service providers to assist with their activities of daily living (e.g., bathing, dressing, feeding) or other personal needs (e.g., employment maintenance, medication access; Jesus et al., 2021). PWD reported being unable to receive support services because of COVID-19 social distancing precautions and protocol provided by the Centers for Disease Control and Prevention (Centers for Disease Control and Prevention, n.d.-b; Jesus et al., 2021). PWD frequently use supported employment services to obtain and maintain integrated employment (Drake et al., 2021). COVID-19 caused a disruption in the delivery of supported employment and/or other employment-related support services. PWD (e.g., MS, SCI) transitioned to remote work, while others reported difficulty accessing consistent support services due to social distancing restrictions (Na & Yang, 2022; Sheppard-Jones, Avellone, et al., 2021; Vives Alvarado et al., 2021).
The COVID-19 pandemic can be classified as an adverse event because, according to the Substance Abuse and Mental Health Services Administration (SAMHSA, 2022), major adverse events have the potential to cause catastrophic loss of life or destruction. When an adverse event occurs, PWD may not have sufficient resources for recovery. During the 2008 economic crisis, persons with disabilities, compared to persons without disabilities, reported more extended periods of unemployment and a more remarkable inability to recover from financial hardships (Bengali et al., 2021; Fogg et al., 2010; Livermore & Honeycutt, 2015; McAlpine & Alang, 2020). Among persons affected by Hurricane Katrina, PWD reported an inability to recover from financial hardship because of their job loss status and inability to obtain employment compared to employment opportunities pre-Katrina (Stough et al., 2016). When providing VR or other employment-related services, counselors should consider the impact of long-term unemployment and inconsistent service delivery. Through understanding the experiences of PWD during COVID-19, counselors can enhance service delivery methods and ensure individuals receive appropriate services to fit their needs. VR counselors can support PWD through instruction in self-advocacy or career pathways using services such as guidance and counseling. Through instruction in self-advocacy, VR counselors facilitate empowerment for an individual’s level of independence when needing to request job accommodations or support with remote work, most likely to occur when an individual is no longer receiving VR services but finds themselves in need of support. The career pathways approach enables an individual to gain work experience and determine essential training (e.g., certification, degree, diploma, vocational training) to reach a long-term job goal and decrease the likelihood of job loss during adverse events (D. Schwartz et al., 2018).
Second, within the grouping of quality of life, the relationship between perceived quality of life during COVID-19 was reported across several studies. During COVID-19, PWD reported limited access to COVID-19 information, the use of social media to exchange information with others, and disruptions in media provider services (e.g., service delays, service cancellations). Communities usually depend upon trustworthy information during a crisis or adverse event (Roberts et al., 2021). Regarding digital communication for COVID-19 information in the U.S., the majority of adults reported using e-mail or other messaging services to communicate about the virus (Statista Research Department, 2021). However, during the pandemic, many platforms experienced irregular, outdated, incorrect, or inaccessible information (Goggin & Ellis, 2020). The dissemination of COVID-19 information (e.g., number of cases, social distancing protocols, vaccine information) was often convoluted with a mixture of true and false information; this likely resulted from a need to publish information quickly and the difficulty in verifying or reviewing all types of information (e.g., social media; Mheidly & Fares, 2020).
Throughout the COVID-19 pandemic, the use of social media has been referred to as an “infodemic,” noting that information regarding the illness and vaccine-related information predominately stems from the antivaccination community, and little input exists from the medical community (Hernandez et al., 2021). When addressing COVID-19-related information and communication access among PWD, it is essential to consider the effect of past adverse events on PWD. Natural disasters (e.g., hurricanes, earthquakes, floods, epidemics) impact PWD at higher rates than persons without disabilities (Battle, 2015). During Hurricane Katrina, many individuals, including PWD, had limited or no ability to receive messages about evacuation, access transportation for evacuation, or obtain services to meet basic needs. During adverse events, including natural disasters, people with disabilities report being unsure about whom to contact regarding disaster preparedness or relief (Fox et al., 2010). During the 2018-2019 Ebola outbreak in the eastern Democratic Republic of the Congo, the abundance of incorrect information presented through the communication systems often inhibited the ability for behavior changes through mitigation efforts and a reduction in the spread of the disease. This was also reported as facilitating a lack of trust in communication systems (Vinck et al., 2019).
When providing employment-related support services, VR counselors or other professionals should provide support to ensure PWD have access to necessary information related to an event. The use of services such as guidance and counseling or a check-in phone call or email can ensure the client is safe and receiving accurate information, and can respond appropriately to the event. Checking in with recipients of services ensures accurate and trustworthy information is being received, while also ensuring individuals receive the necessary supports to access information or participate in social media. Sending out communication to clients through an agency or organizational statement presents consistent information and can support clients who are unsure where to turn for trustworthy information. Training material on topics such as social media use can potentially enhance safe usage across various platforms (e.g., Twitter, Facebook, Instagram) while also increasing access to reliable information. Similar training provided within the constructs of a job club may be beneficial for clients in order to prepare for adverse events. Presenting topics such as safe social media usage, communication strategies, or employment planning provides options for individuals to maintain independence, especially if they are not actively receiving VR services.
Finally, within the grouping of coping, the relationship between COVID-19 and continuous stress was reported across several studies. Among PWD during COVID-19, stress was reported as associated with job loss, housing stability, access to health care, and lower levels of well-being. Ciciurkaite et al. (2021) recognized COVID-19 as a stressor, but also acknowledged that PWD are likely to experience stress at a more significant level due to additional stressors (e.g., loss of income, inability to pay for basic needs, health insurance). The National Governor’s Association (NGA, n.d.) reported that, during the early months of COVID-19 (March to April 2020), “the number of employed working age-people with disabilities fell by 20%” (p. 1). This trend of increased job loss continued throughout 2020 and 2021 and, as a population, PWD were more likely to experience unemployment compared to persons without disabilities (U.S. Bureau of Labor Statistics, 2022). Unemployed persons and persons who experience job loss, compared to employed persons, report higher levels of psychological distress and higher levels of depression (Hergenrather et al., 2015). Individuals with intellectual and developmental disabilities were noted as a population at a heightened risk for severe effects from COVID-19, and many individuals reported that COVID-19 had a “negative impact” on their lives, increasing levels of stress and decreasing levels of life satisfaction (Fisher et al., 2022, p. 6).
Housing, a reported social determinant of health, and related housing concerns are presented as additional stressors for PWD throughout COVID-19 (Jesus et al., 2021; Rolfe et al., 2020). The National Council on Disability (NCD, 2021) reported that COVID-19 created housing issues for many individuals, specifically a lack of accessible housing subsidies leaving “nearly 400,000 people with disabilities living in the streets, in shelters” (p. 101). Jesus et al. (2021) noted that, as a response to the COVID-19 social distancing restrictions, PWD experienced disproportionate rates of job loss, thus increasing financial stressors as well as housing and food insecurities. In February 2022, the White House released a fact sheet to address the needs of PWD, noting efforts to develop accessible at-home tests, increase the availability of testing guidance in American Sign Language, and launch a disability access line to support individuals with testing needs. Additionally, the NCD (2021) developed a report addressed to the President of the United States, stating that PWD disproportionately experienced negative impact due to COVID-19. In it, they made note that individuals “were denied assistance of critical support persons during hospital stays” (p. 2), specific disability populations (e.g., deaf, hard of hearing, deaf-blind, blind) experienced disruptions in communication as a result of mandated mask-wearing, and that adjustments made over the course of COVID-19 (e.g., financial, social, familial) impacted PWD and their mental health.
Throughout the COVID-19 pandemic, PWD in the U.S. reported experiencing higher levels of stress and worry, explicitly regarding access to medical care, housing, financial stability, and food availability (Wang et al., 2022). PWD disproportionately experienced increased mental health concerns and decreased well-being (Nerlich et al., 2021; Wang et al., 2022). Additionally, PWD faced “barriers and concerns during the COVID-19 pandemic as a result of longstanding and pervasive systemic ableism that places them at risk for additional stress and trauma” (Lund et al., 2020, p. 319). These mental health concerns included increased anxiety and depression (Nieweglowski & Sheehan, 2021; Wang et al., 2022), increased substance use (Rumrill et al., 2021), and worsened health outcomes because of increased social isolation and loneliness (Luchetti et al., 2020; Rumrill et al., 2021).
Among PWD, the experience of stress related to an adverse event was not limited to COVID-19. After Hurricane Katrina, PWD were faced with disruptions to several components of independent living (e.g., employment, medical care, housing, transportation), and even though many responded with resiliency, this adverse event shed light on the interconnectedness between people and their environments (Fox et al., 2010). In additional research specific to the result of Hurricane Katrina, Stough et al. (2016) reported that PWD experienced significant barriers to recovery in various areas of living (e.g., housing, employment, health, transportation) and noted increased levels of anxiety and worry as their needs were not met. When considering the impact to PWD during adverse events, it is essential to consider their needs, especially in terms of comprehending or accessing the presented information regarding the event (Battle, 2015). VR counselors and other professionals may benefit from additional information and heightened awareness regarding the needs of PWD in preparation for adverse events. By understanding how PWD respond to adverse events and potential barriers during adverse events, VR counselors are better equipped to tailor services to individual needs, such as arranging independent living services or providing training for financial empowerment.
Individuals with and without disabilities experienced considerable increases in stress and trauma throughout COVID-19. As a result, many individuals experienced increased rates of mental health concerns, frequency of substance use, and suicidality. Although there is much-published literature addressing coping and self-care, it is limited when addressing PWD. Lee et al. (2021) reported that COVID-19-related stress is significantly related to maladaptive COVID-19 coping. Identified maladaptive coping methods were reported as substance use, avoidance, social isolation, and lack of awareness (Czeisler et al., 2021; Lee et al., 2021; Umucu & Lee, 2020).
When engaging in employment-related services, it is crucial for VR counselors to consider an individual’s ability to cope with stress or stressful events. To support the implementation of adaptive coping skills, VR counselors could offer VR participants training on the importance of active coping. Providing this level of support potentially reduces an individual’s likelihood of engaging in maladaptive coping, such as using substances for coping. VR counselors can utilize guidance and counseling methods to provide individual sessions for teaching coping skills or group counseling methods to support multiple clients who wish to develop coping skills. Using group counseling methods also potentially helps create peer support groups, where individuals gain coping skills and social support.
Because of limited research addressing how PWD experience stress or reflect on how adverse events can negatively impact their lives, the authors applied the results of this systematic review of literature to develop the COVID-19 Lived Experiences Scale for Persons with Disabilities (CLES-PWD) (see Table 2). The purpose of this scale is to support VR counselors and community service providers in holistically understanding the impact of the COVID-19 pandemic and the experiences of PWD. This structured interview scale enables PWD to self-reflect on their experiences during the COVID-19 pandemic and also thoroughly discuss these experiences with professionals. The CLES-PWD addresses employment, quality of life, and coping. Using this scale with individuals receiving VR services may assist in providing targeted service delivery and developing the Individualized Plan for Employment (IPE). The CLES-PWD provides PWD with a prompt from which to construct a response from lived experiences and assure that relevant issues are covered (O’Cathain & Thomas, 2004).
Implications of Findings
The overall goal of the CLES-PWD is to enhance insight for PWD to self-determine how significantly the COVID-19 pandemic impacted their daily lives. For example, because persons with less than a four-year degree were most likely to experience employment changes (e.g., reduction in hours, job loss, furlough) during COVID-19, it may benefit a person with a high school diploma to complete a certificate-type program or a college degree. Throughout COVID-19, PWD noted significant barriers to accessing services, or disruptions in services; additionally, many individuals experienced increased levels of stress and difficulty developing healthy coping skills. Implementation of the CLES-PWD provides VR counselors, community service providers, and PWD an opportunity to reflect on adaptive and maladaptive coping skills to develop a plan for addressing stress.
Another consideration for PWD diagnosed with COVID-19 is the presentation of long COVID. Long COVID endures for weeks or months after the initial COVID-19 infection, bringing a range of new or ongoing symptoms and worsening physical or mental activity (Stephenson, 2021). In July 2021, long COVID was covered under Section 504 of the ADA, qualifying as a physiological condition affecting one or more body systems (U.S. Department of Health Services, 2021). There is limited research on the trajectory of long COVID or its impact on PWD; worry and uncertainty present themselves as individuals try to navigate the unpredictability of fluctuating symptoms (Brown & O’Brien, 2021). Jesus et al. (2020) described the challenges and inequities PWD experienced throughout COVID-19, noting that decisions made regarding social distance protocols, or the re-opening of communities, disproportionately affected marginalized populations. Rotarou et al. (2021) defined the term disablism as “those discourses and practices that exclude, discriminate against, and oppress disabled people,” essentially devaluing their presence or this need for “self-protection” (p. 1). Lund et al. (2020) highlighted the trauma response for PWD throughout COVID-19 and described ongoing accessibility issues with medical care as a possible trigger. Implementing the CLES-PWD as a routine discussion protocol during the employment plan development process can assist with identifying at-risk areas based on an individual’s desired employment or current coping strategies during future adverse events.
Limitations
Findings reported in this systematic review of literature are subject to limitations. First, even though all studies reported disability as a demographic component of the study, this information was self-reported. In addition to self-reported disability, the literature was not inclusive of all disabilities and some generalized disabilities or chronic illnesses. Second, an unequal number of qualitative and quantitative studies were used as part of this systematic review, thus potentially skewing the identified themes. Third, among research discussing employment loss for PWD during COVID-19, there is a lack of discussion on the use of VR-related services as COVID-19 continues. Fourth, different assessment measures were utilized to determine the impact of COVID-19 on PWD, creating a bias on certain constructs. Also regarding assessment measures, several studies reported creating new assessments to measure the impact of COVID-19 on PWD; however, some of them were not psychometrically validated. Finally, the reporting of underrepresented, minoritized intersections of the identity of PWD was limited within the presented literature. Throughout COVID-19, it is noteworthy to mention that additional stressors, such as racial tensions experienced simultaneously, potentially impact an individual’s ability to cope. Future studies could focus on the impact of COVID-19 on PWD living in rural versus urban areas, and individuals with different racial, ethnic, gender, or sexual identities, as well as how additional stressors (e.g., racial tensions) moderate coping. Although these limitations are presented, this systematic review of literature offers supporting information on the significant impact of COVID-19 and employment, quality of life, and coping for PWD.
Conclusion
Since January 2020, COVID-19 has presented significant disruption with more than one million deaths in the U.S., inconsistent delivery of vaccines, and varying quarantine protocols (CDC n.d.-a). This systematic review of literature aimed to understand the impact of COVID-19 on PWD in targeted areas, including changes in employment status, quality of life, and ability to cope. Findings from this review are consistent with previous research on PWD during adverse events. From the study findings, the CLES-PWD was developed, and can be used as a supplemental tool for VR professionals to assist with employment planning. Often during adverse events, the needs of PWD are disregarded, creating additional barriers or stressors. As VR professionals work to support PWD to obtain integrated employment opportunities, increasing awareness of the likelihood that an adverse event will negatively impact a person presents an opportunity to enhance targeted outcomes. Additional research is needed to determine how the CLES-PWD can be implemented as part of the VR employment planning process and its impact on employment outcomes and adversity preparedness for PWD.